

Improving Cerebral Blood Flow after Arterial Recanalization: A Novel Therapeutic Strategy in Stroke
- PMID: 29232823
- PMCID: PMC5751271
- DOI: 10.3390/ijms18122669
Improving Cerebral Blood Flow after Arterial Recanalization: A Novel Therapeutic Strategy in Stroke
Abstract
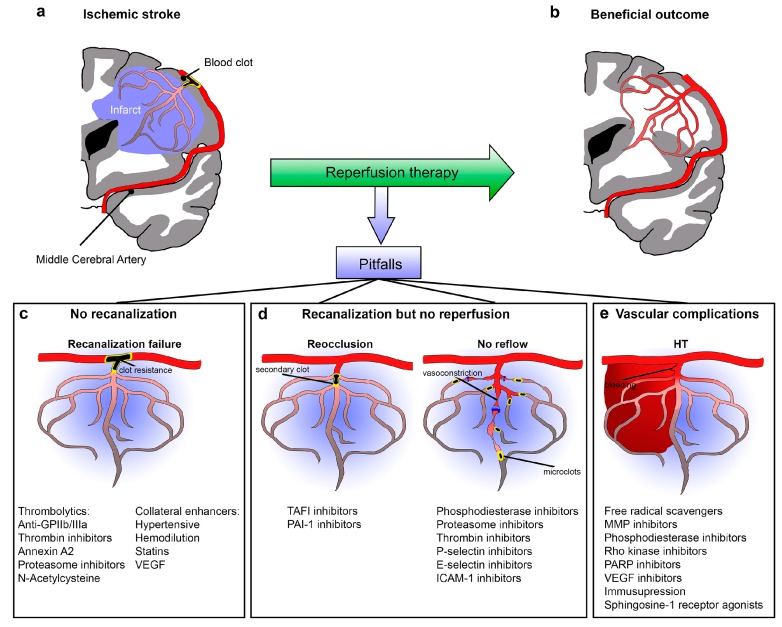
Ischemic stroke is caused by a disruption in blood supply to a region of the brain. It induces dysfunction of brain cells and networks, resulting in sudden neurological deficits. The cause of stroke is vascular, but the consequences are neurological. Decades of research have focused on finding new strategies to reduce the neural damage after cerebral ischemia. However, despite the incredibly huge investment, all strategies targeting neuroprotection have failed to demonstrate clinical efficacy. Today, treatment for stroke consists of dealing with the cause, attempting to remove the occluding blood clot and recanalize the vessel. However, clinical evidence suggests that the beneficial effect of post-stroke recanalization may be hampered by the occurrence of microvascular reperfusion failure. In short: recanalization is not synonymous with reperfusion. Today, clinicians are confronted with several challenges in acute stroke therapy, even after successful recanalization: (1) induce reperfusion, (2) avoid hemorrhagic transformation (HT), and (3) avoid early or late vascular reocclusion. All these parameters impact the restoration of cerebral blood flow after stroke. Recent advances in understanding the molecular consequences of recanalization and reperfusion may lead to innovative therapeutic strategies for improving reperfusion after stroke. In this review, we will highlight the importance of restoring normal cerebral blood flow after stroke and outline molecular mechanisms involved in blood flow regulation.
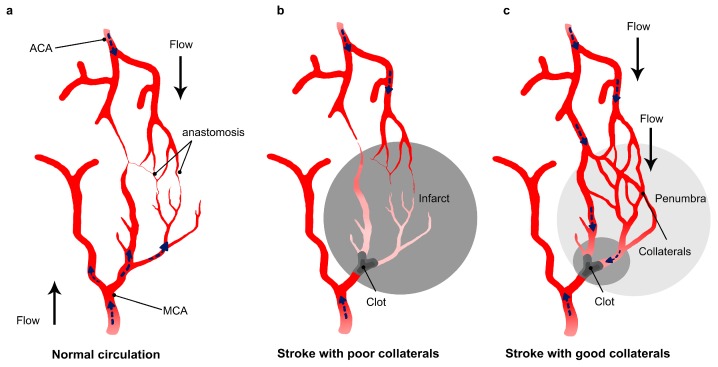
Keywords: collaterals; hemorrhagic transformation; no-reflow and reocclusion; reperfusion; stroke.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- WHO The World Health Report 2002—Reducing Risks, Promoting Healthy Life. [(accessed on 23 July 2012)]; Available online: http://www.who.int/whr/2002/en/
-
- Goyal M., Menon B.K., van Zwam W.H., Dippel D.W.J., Mitchell P.J., Demchuk A.M., Dávalos A., Majoie C.B.L.M., van der Lugt A., de Miquel M.A., et al. HERMES collaborators Endovascular thrombectomy after large-vessel ischaemic stroke: A meta-analysis of individual patient data from five randomised trials. Lancet. 2016;387:1723–1731. doi: 10.1016/S0140-6736(16)00163-X. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
