

Short- and long-term outcomes in infective endocarditis patients: a systematic review and meta-analysis
- PMID: 29233094
- PMCID: PMC5728061
- DOI: 10.1186/s12872-017-0729-5
Short- and long-term outcomes in infective endocarditis patients: a systematic review and meta-analysis
Erratum in
-
Correction to: Short- and long-term outcomes in infective endocarditis patients: a systematic review and meta-analysis.BMC Cardiovasc Disord. 2018 Jan 12;18(1):5. doi: 10.1186/s12872-018-0742-3. BMC Cardiovasc Disord. 2018. PMID: 29329514 Free PMC article.
Abstract
Background: Despite advances in medical knowledge, technology and antimicrobial therapy, infective endocarditis (IE) is still associated with devastating outcomes. No reviews have yet assessed the outcomes of IE patients undergoing short- and long-term outcome evaluation, such as all-cause mortality and IE-related complications. We conducted a systematic review and meta-analysis to examine the short- and long-term mortality, as well as IE-related complications in patients with definite IE.
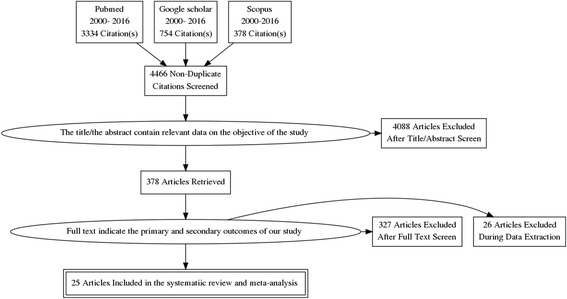
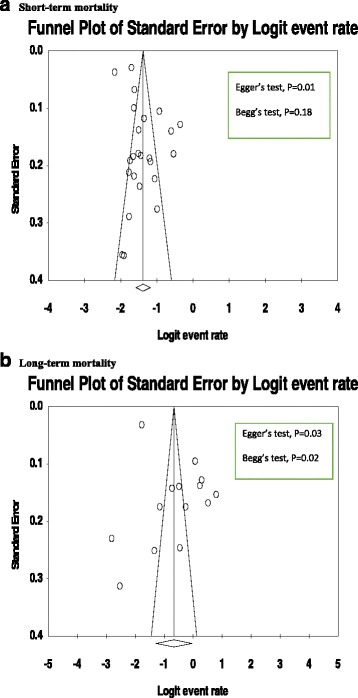
Methods: A computerized systematic literature search was carried out in PubMed, Scopus and Google Scholar from 2000 to August, 2016. Included studies were published studies in English that assessed short-and long-term mortality for adult IE patients. Pooled estimations with 95% confidence interval (CI) were calculated with DerSimonian-Laird (DL) random-effects model. Sensitivity and subgroup analyses were also performed. Publication bias was evaluated using inspection of funnel plots and statistical tests.
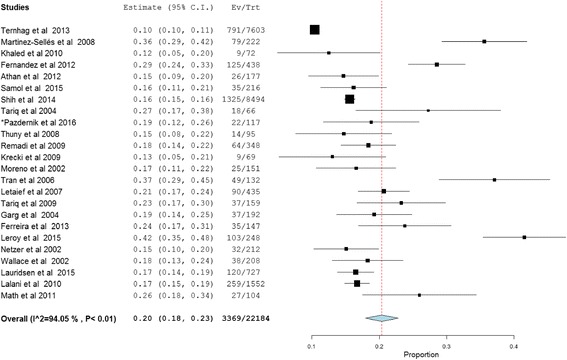
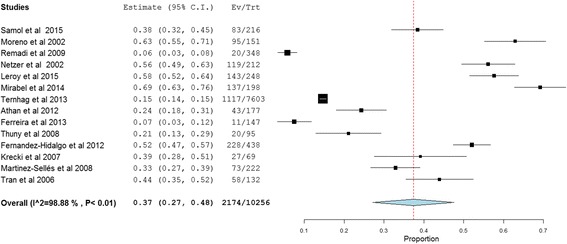
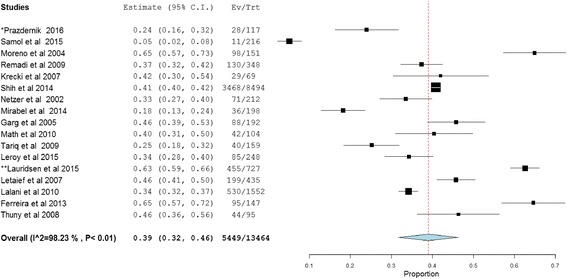
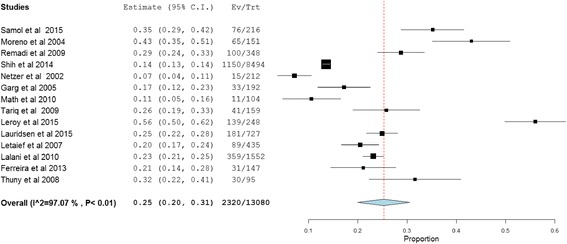
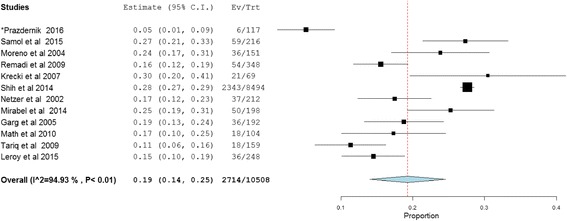
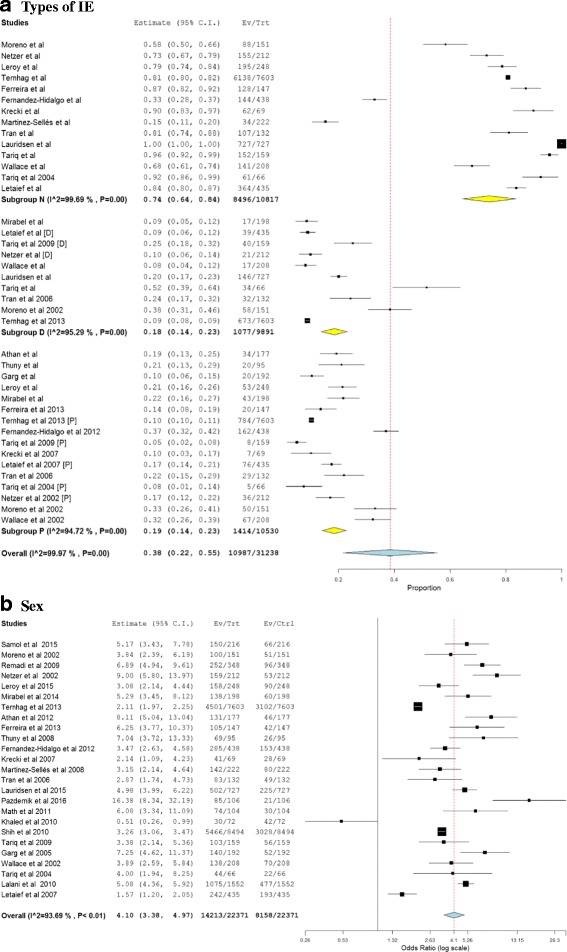
Results: Twenty five observational studies (retrospective, 14; prospective, 11) including 22,382 patients were identified. The overall pooled mortality estimates for IE patients who underwent short- and long-term follow-up were 20% (95% CI: 18.0-23.0, P < 0.01) and 37% (95% CI: 27.0-48.0, P < 0.01), respectively. The pooled prevalence of cardiac complications in patients with IE was found to be 39% (95%CI: 32.0-46.0) while septic embolism and renal complications accounted for 25% (95% CI: 20.0-31) and 19% (95% CI: 14.0-25.0) (all P < 0.01), respectively.
Conclusion: Irrespective of the follow-up period, a significantly higher mortality rate was reported in IE patients, and the burden of IE-related complications were immense. Further research is needed to assess the determinants of overall mortality in IE patients, as well as well-designed observational studies to conform our results.
Keywords: Infective endocarditis; Long-term mortality; Meta-analysis; Short-term mortality.
Conflict of interest statement
Ethics approval and consent to participate
Our study is an investigation of the literature and does not need ethical approval for retrieving the already available public content.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
