

Decompressive craniectomy in traumatic brain injury: usage and clinical outcome in a single centre
- PMID: 29234973
- PMCID: PMC5766728
- DOI: 10.1007/s00701-017-3418-3
Decompressive craniectomy in traumatic brain injury: usage and clinical outcome in a single centre
Abstract
Background: Two randomised controlled trials (RCTs) of decompressive craniectomy (DC) in traumatic brain injury (TBI) have shown poor outcome, but there are considerations of how these protocols relate to real practice. The aims of this study were to evaluate usage and outcome of DC and thiopental in a single centre.
Method: The study included all TBI patients treated at the neurointensive care unit, Akademiska sjukhuset, Uppsala, Sweden, between 2008 and 2014. Of 609 patients aged 16 years or older, 35 treated with DC and 23 treated with thiopental only were studied in particular. Background variables, intracranial pressure (ICP) measures and global outcome were analysed.
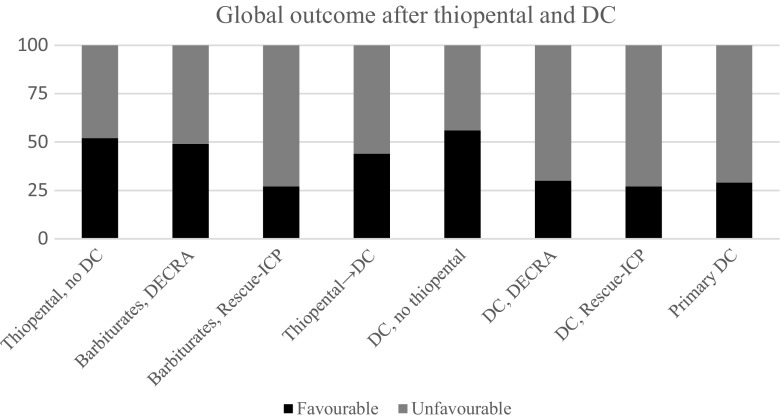
Results: Of 35 DC patients, 9 were treated stepwise with thiopental before DC, 9 were treated stepwise with no thiopental before DC and 17 were treated primarily with DC. Six patients received thiopental after DC. For 23 patients, no DC was needed after thiopental. Eighty-eight percent of our DC patients would have qualified for the DECRA study and 38% for the Rescue-ICP trial. Favourable outcome was 44% in patients treated with thiopental before DC, 56% in patients treated with DC without prior thiopental, 29% in patients treated primarily with DC and 52% in patients treated with thiopental with no DC.
Conclusions: The place for DC in TBI management must be evaluated better, and we believe it is important that future RCTs should have clearer and less permissive ICP criteria regarding when thiopental should be followed by DC and DC followed by thiopental.
Keywords: Decompressive craniectomy; Neurointensive care; Standardised treatment protocol; Thiopental; Traumatic brain injury.
Conflict of interest statement
Conflicts of interest
The authors declare that they have no conflict of interest.
Research involving human participants and animals
All procedures performed in studies involving humans were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. This article does not contain any studies with animals performed by any of the authors.
Informed consent
Informed consent was obtained from the relatives of all participating patients.
Figures
Comment in
-
Decompressive craniectomy in traumatic brain injury-the discussion must continue.Acta Neurochir (Wien). 2018 Jun;160(6):1303. doi: 10.1007/s00701-018-3534-8. Epub 2018 Apr 16. Acta Neurochir (Wien). 2018. PMID: 29658060 No abstract available.
-
Is decision-making easier post RESCUE ICP trial?Acta Neurochir (Wien). 2018 Jun;160(6):1301-1302. doi: 10.1007/s00701-018-3533-9. Epub 2018 Apr 23. Acta Neurochir (Wien). 2018. PMID: 29687252 No abstract available.
References
-
- Compagnone C, Murray GD, Teasdale GM, Maas AI, Esposito D, Princi P, et al. The management of patients with intradural post-traumatic mass lesions: a multicenter survey of current approaches to surgical management in 729 patients coordinated by the European brain injury consortium. Neurosurgery. 2005;57:1183–1192. doi: 10.1227/01.NEU.0000186239.10915.09. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
