

Association of Whole Blood Tacrolimus Concentrations with Kidney Injury in Heart Transplantation Patients
- PMID: 29236211
- PMCID: PMC5956048
- DOI: 10.1007/s13318-017-0453-7
Association of Whole Blood Tacrolimus Concentrations with Kidney Injury in Heart Transplantation Patients
Abstract
Background and objectives: Acute kidney injury (AKI) is frequently observed after heart transplantation and is associated with morbidity and mortality. However, many confounding factors also contribute to the development of AKI in heart transplants. We hypothesized that supratherapeutic whole-blood tacrolimus trough concentrations are associated with AKI.
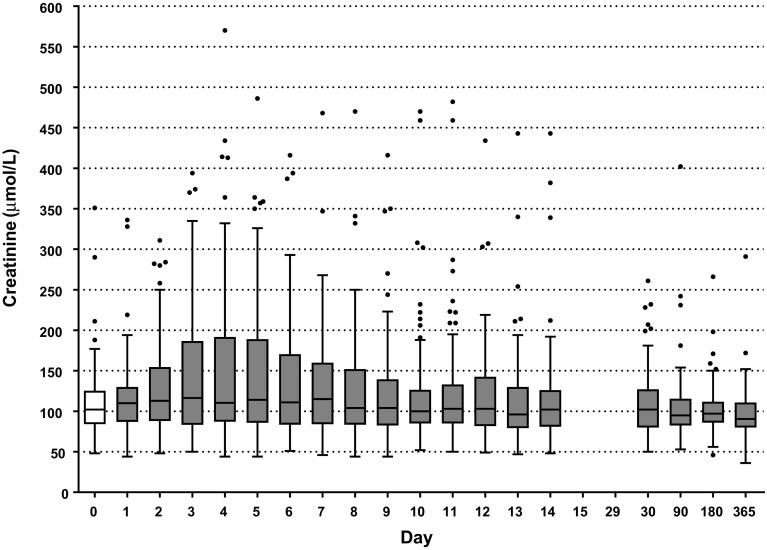
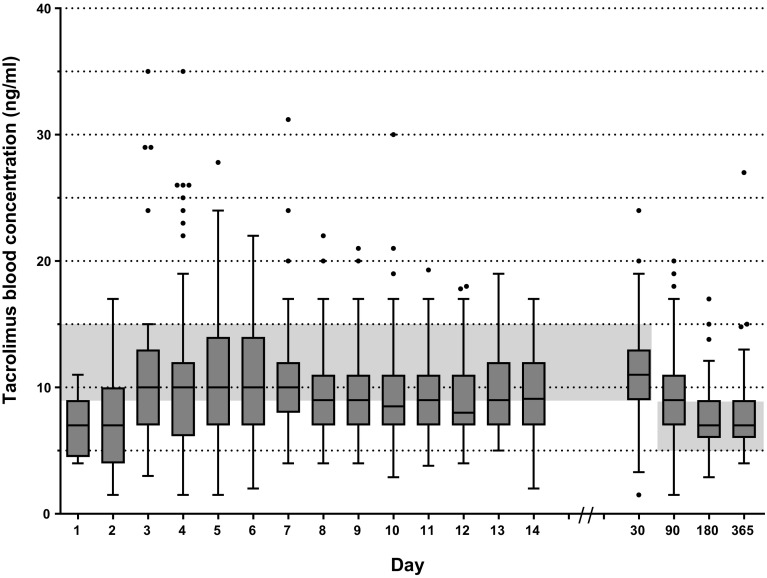
Methods: In a retrospective observational cohort from April 2005 to December 2012, all adult heart transplantation patients were included. AKI was assessed in the first 2 weeks after transplantation as classified by the Kidney Disease Improving Global Outcomes Network (KDIGO). Whole-blood tacrolimus trough concentrations were determined from day 1 to day 14 and at 1, 3, 6 and 12 months post-transplantation. The therapeutic range was 9 to 15 ng/ml in the first 2 months and tapered to 5-8 ng/ml thereafter. The relationship between supratherapeutic tacrolimus trough concentrations and AKI was evaluated. The impact of various potentially confounding factors on tacrolimus concentrations and AKI was considered.
Results: We included 110 patients. AKI occurred in 57% of patients in the first week. Recovery from AKI was seen in 24%. The occurrence of chronic kidney disease (CKD) was 19% at 1 year. Whole-blood tacrolimus trough concentrations were often supratherapeutic and, despite correction for confounding factors, independently associated with AKI (OR 1.66; 95% CI 1.20-2.31).
Conclusions: Supratherapeutic whole-blood tacrolimus trough concentrations are independently associated with the development of AKI in adult heart transplantation patients. More stringent dosing of tacrolimus early after transplantation may be critical in preserving the kidney function.
Conflict of interest statement
Ethics
This study was conducted in compliance with the Declaration of Helsinki, Good Clinical Practice guidelines and in accordance with local and national regulatory requirements and laws. The accredited ethics committee of the University Medical Center Utrecht has approved of the use of patient data (IRB UMC Utrecht protocol number 12-071).
Disclosure of interest
Claudine C. Hunault, Marianne C. Verhaar, Johannes H. Kirkels, Jozef Kesecioglu and Dylan W. de Lange declare that they have no conflicts of interest.
Funding
No source of funding was used to conduct this study.
Figures
References
-
- Stehlik J, Edwards LB, Kucheryavaya AY, Benden C, Christie JD, Dipchand AI, et al. The Registry of the International Society for Heart and Lung Transplantation: 29th official adult heart transplant report–2012. J Heart Lung Transpl. 2012;31:1052–1064. doi: 10.1016/j.healun.2012.08.002. - DOI - PubMed
-
- Guethoff S, Meiser BM, Groetzner J, Eifert S, Grinninger C, Ueberfuhr P, et al. Ten-year results of a randomized trial comparing tacrolimus versus cyclosporine a in combination with mycophenolate mofetil after heart transplantation. Transplantation. 2013;95:629–634. doi: 10.1097/TP.0b013e318277e378. - DOI - PubMed
-
- Penninga L, Møller CH, Gustafsson F, Steinbrüchel DA, Gluud C. Tacrolimus versus cyclosporine as primary immunosuppression after heart transplantation: systematic review with meta-analyses and trial sequential analyses of randomised trials. Eur J Clin Pharmacol. 2010;66:1177–1187. doi: 10.1007/s00228-010-0902-6. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
