

Recent Trends in Chemotherapy Use and Oncologists' Treatment Recommendations for Early-Stage Breast Cancer
- PMID: 29237009
- PMCID: PMC5946952
- DOI: 10.1093/jnci/djx239
Recent Trends in Chemotherapy Use and Oncologists' Treatment Recommendations for Early-Stage Breast Cancer
Abstract
Background: There is growing concern about overtreatment of breast cancer as outcomes have improved over time. However, little is known about how chemotherapy use and oncologists' recommendations have changed in recent years.
Methods: We surveyed 5080 women (70% response rate) diagnosed with breast cancer between 2013 and 2015 and accrued through two Surveillance, Epidemiology, and End Results registries (Georgia and Los Angeles) about chemotherapy receipt and their oncologists' chemotherapy recommendations. We surveyed 504 attending oncologists (60.3% response rate ) about chemotherapy recommendations in node-negative and node-positive case scenarios. We conducted descriptive statistics of chemotherapy use and patients' report of oncologists' recommendations and used a generalized linear mixed model of chemotherapy use according to time and clinical factors. All statistical tests were two-sided.
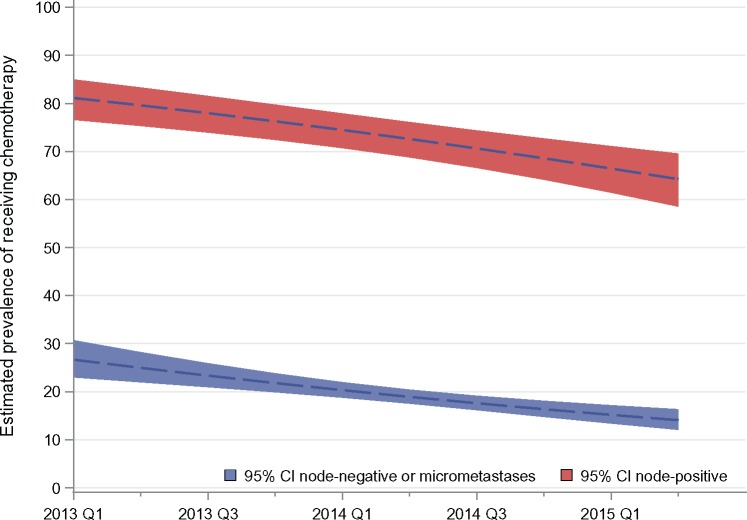
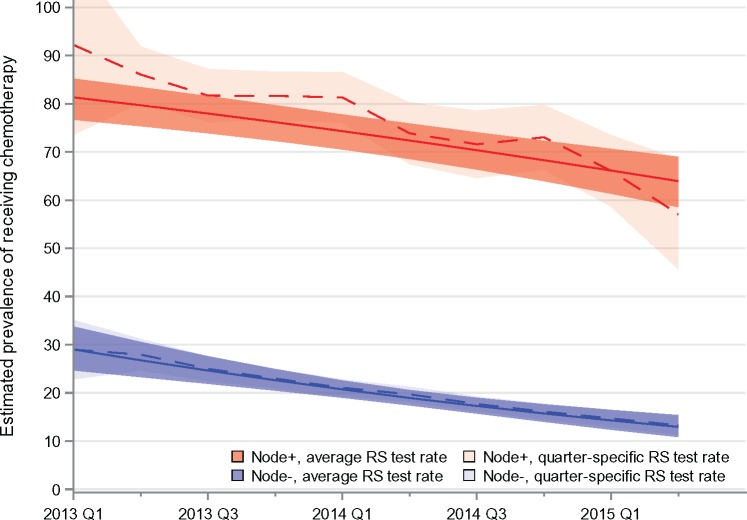
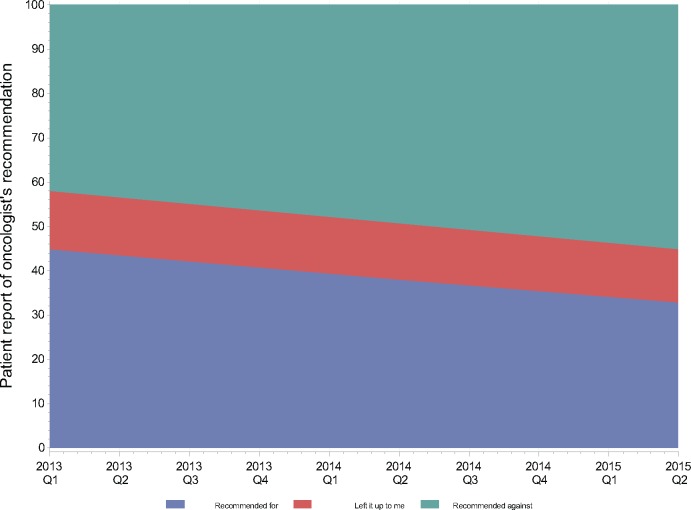
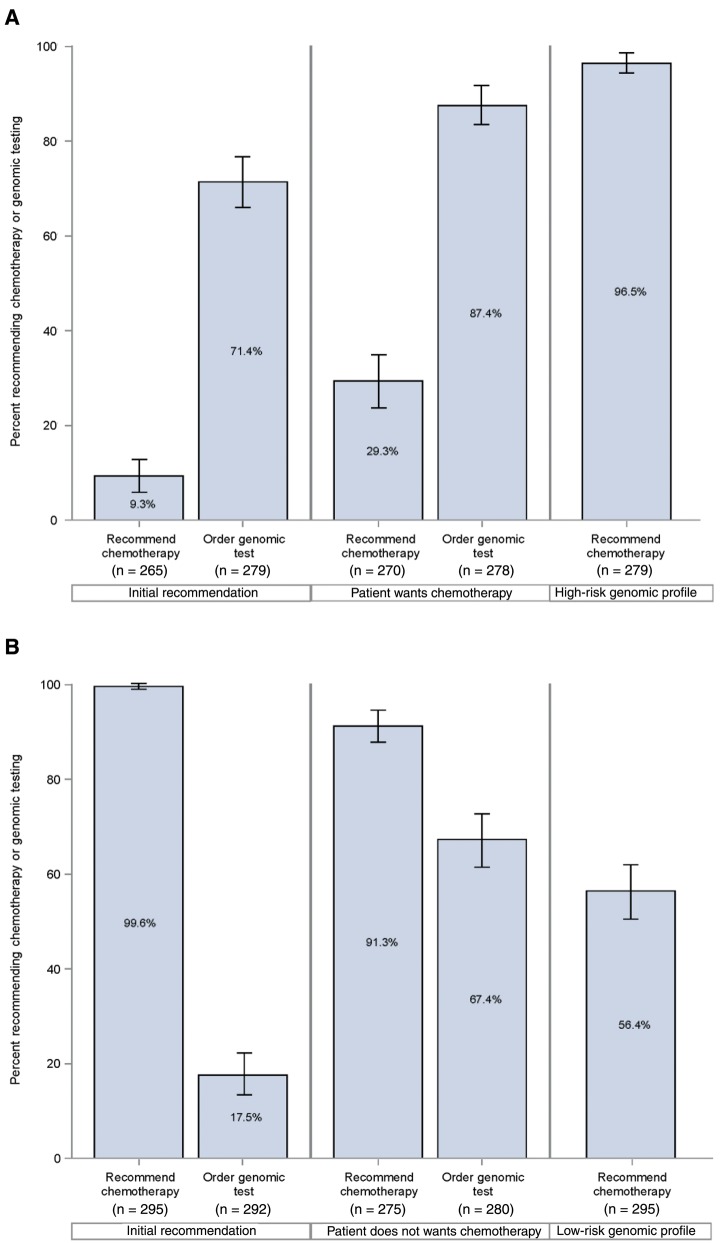
Results: The analytic sample was 2926 patients with stage I-II, estrogen receptor-positive, human epidermal growth factor receptor 2-negative breast cancer. From 2013 to 2015, keeping other factors constant, chemotherapy use was estimated to decline from 34.5% (95% confidence interval [CI] = 30.8% to 38.3%) to 21.3% (95% CI = 19.0% to 23.7%, P < .001). Estimated decline in chemotherapy use was from 26.6% (95% CI = 23.0% to 30.7%) to 14.1% (95% CI = 12.0% to 16.3%) for node-negative/micrometastasis patients and from 81.1% (95% CI = 76.6% to 85.0%) to 64.2% (95% CI = 58.6% to 69.6%) for node-positive patients. Use of the 21-gene recurrence score (RS) did not change among node-negative/micrometastasis patients, and increasing RS use in node-positive patients accounted for one-third of the chemotherapy decline. Patients' report of oncologists' recommendations for chemotherapy declined from 44.9% (95% CI = 40.2% to 49.7%) to 31.6% (95% CI = 25.9% to 37.9%), controlling for other factors. Oncologists were much more likely to order RS if patient preferences were discordant with their recommendations (67.4%, 95% CI = 61.7% to 73.0%, vs 17.5%, 95% CI = 13.1% to 22.0%, concordant), and they adjusted recommendations based on patient preferences and RS results.
Conclusions: For both node-negative/micrometastasis and node-positive patients, chemotherapy receipt and oncologists' recommendations for chemotherapy declined markedly over time, without substantial change in practice guidelines. Results of ongoing trials will be essential to confirm the quality of this approach to breast cancer care.
Figures
Comment in
-
Adjuvant Chemotherapy for ER+ Breast Cancer: A Sea Change is Underway.J Natl Cancer Inst. 2018 May 1;110(5):443-445. doi: 10.1093/jnci/djx264. J Natl Cancer Inst. 2018. PMID: 29237035 No abstract available.
References
-
- Paik S, Shak S, Tang G et al. , A multigene assay to predict recurrence of tamoxifen-treated, node-negative breast cancer. N Engl J Med. 2004;351(27):2817–2826.http://dx.doi.org/10.1056/NEJMoa041588 - DOI - PubMed
-
- Paik S, Tang G, Shak S et al. , Gene expression and benefit of chemotherapy in women with node-negative, estrogen receptor-positive breast cancer. J Clin Oncol. 2006;24(23):3726–3734.http://dx.doi.org/10.1200/JCO.2005.04.7985 - DOI - PubMed
-
- Sparano JA, Gray RJ, Makower DF et al. , Prospective validation of a 21-gene expression assay in breast cancer. N Engl J Med. 2015;373(21):2005–2014.http://dx.doi.org/10.1056/NEJMoa1510764 - DOI - PMC - PubMed
-
- Perou CM, Sorlie T, Eisen MB et al. , Molecular portraits of human breast tumours. Nature. 2000;406(6797):747–752.http://dx.doi.org/10.1038/35021093 - DOI - PubMed
-
- Gradishar WJ, Anderson BO, Balassanian R et al. , Invasive breast cancer version 1.2016, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw. 2016;14(3):324–354.http://dx.doi.org/10.6004/jnccn.2016.0037 - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
