

Clinical implications of Plasmodium resistance to atovaquone/proguanil: a systematic review and meta-analysis
- PMID: 29237012
- PMCID: PMC5890752
- DOI: 10.1093/jac/dkx431
Clinical implications of Plasmodium resistance to atovaquone/proguanil: a systematic review and meta-analysis
Abstract
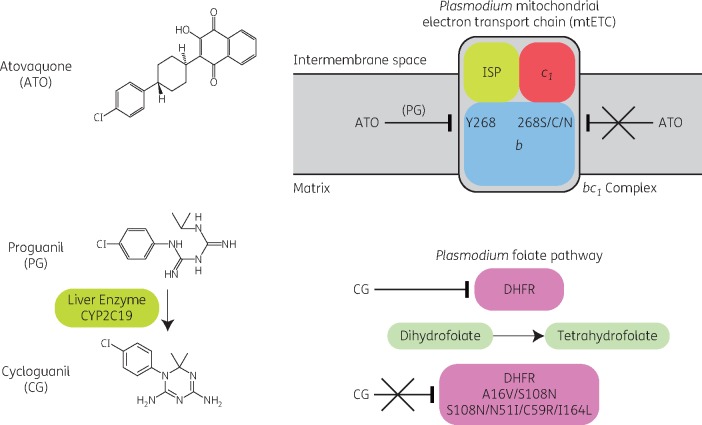
Background: Atovaquone/proguanil, registered as Malarone®, is a fixed-dose combination recommended for first-line treatment of uncomplicated Plasmodium falciparum malaria in non-endemic countries and its prevention in travellers. Mutations in the cytochrome bc1 complex are causally associated with atovaquone resistance.
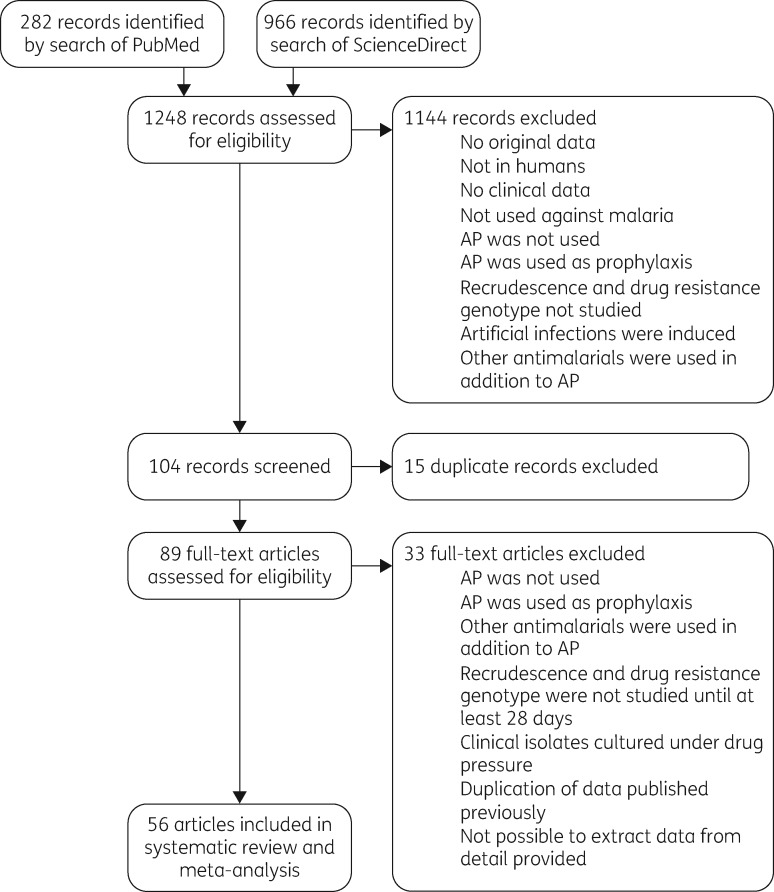
Methods: This systematic review assesses the clinical efficacy of atovaquone/proguanil treatment of uncomplicated malaria and examines the extent to which codon 268 mutation in cytochrome b influences treatment failure and recrudescence based on published information.
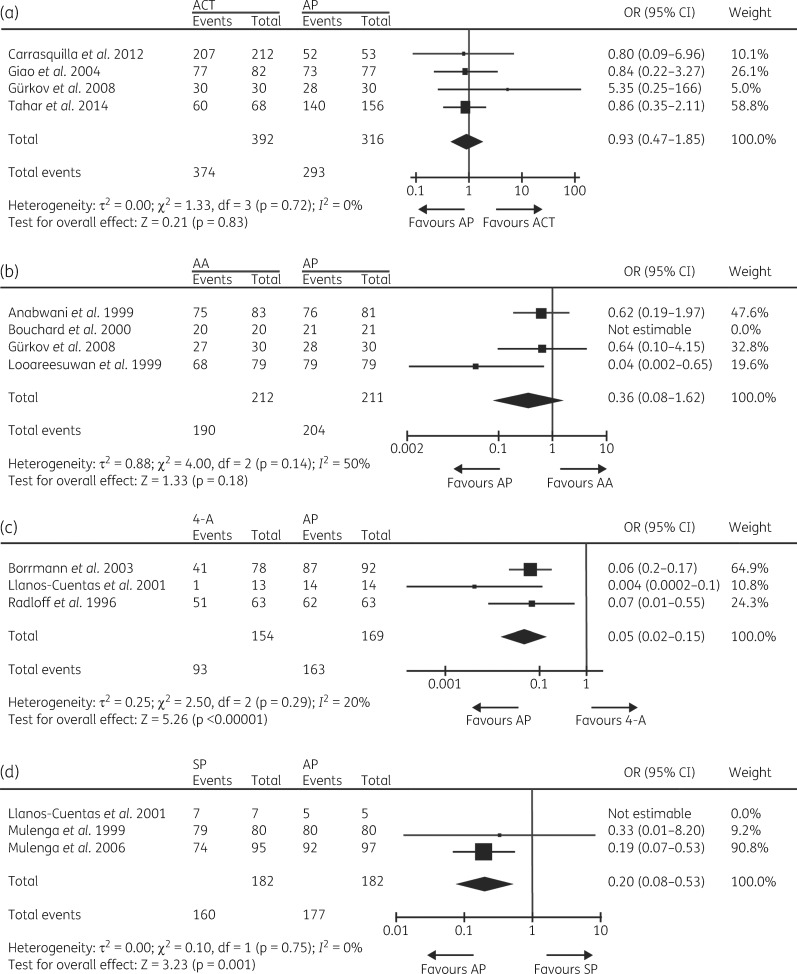
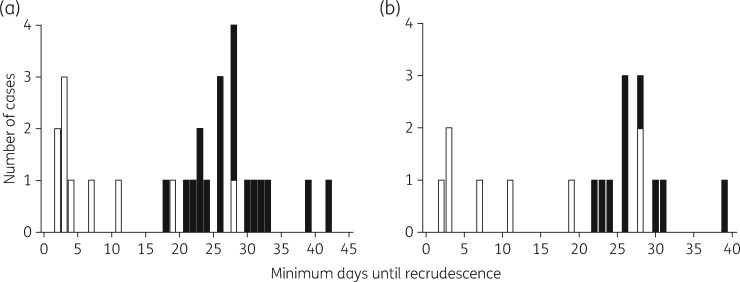
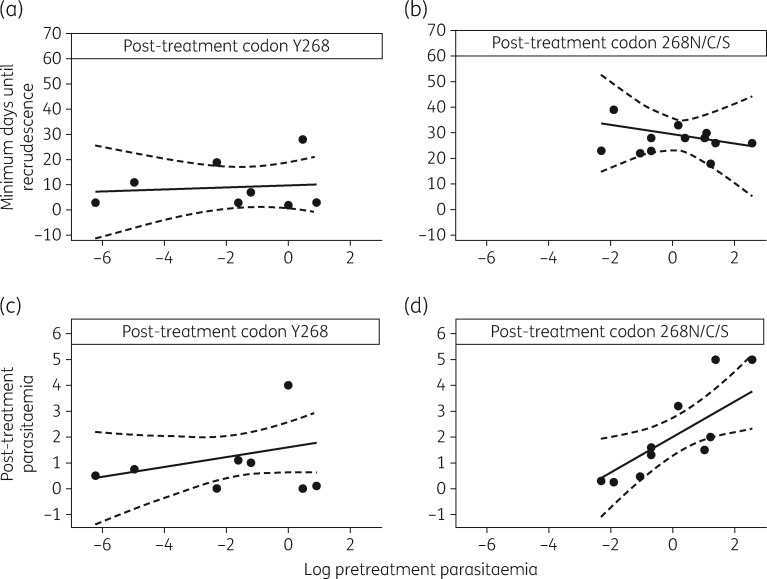
Results: Data suggest that atovaquone/proguanil treatment efficacy is 89%-98% for P. falciparum malaria (from 27 studies including between 18 and 253 patients in each case) and 20%-26% for Plasmodium vivax malaria (from 1 study including 25 patients). The in vitro P. falciparum phenotype of atovaquone resistance is an IC50 value >28 nM. Case report analyses predict that recrudescence in a patient presenting with parasites carrying cytochrome b codon 268 mutation will occur on average at day 29 (95% CI: 22, 35), 19 (95% CI: 7, 30) days longer than if the mutation is absent.
Conclusions: Evidence suggests atovaquone/proguanil treatment for P. falciparum malaria is effective. Late treatment failure is likely to be associated with a codon 268 mutation in cytochrome b, though recent evidence from animal models suggests these mutations may not spread within the population. However, early treatment failure is likely to arise through alternative mechanisms, requiring further investigation.
Figures
References
-
- WHO. Guidelines for the Treatment of Malaria, Third Edition 2015. http://www.who.int/malaria/publications/atoz/9789241549127/en/.
-
- WHO. World Malaria Report 2016 2016. http://www.who.int/malaria/publications/world-malaria-report-2016/en/.
-
- Krishna S, Kremsner PG.. Antidogmatic approaches to artemisinin resistance: reappraisal as treatment failure with artemisinin combination therapy. Trends Parasitol 2013; 29: 313.. - PubMed
-
- WHO. Update on Artemisinin Resistance—April 2012 2012. http://www.who.int/malaria/publications/atoz/updateartemsininresistancea....
-
- PHE. Guidelines for Malaria Prevention in Travellers from the UK 2017. https://www.gov.uk/government/publications/malaria-prevention-guidelines....
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
