

High-flow nasal cannula oxygen therapy versus conventional oxygen therapy in patients with acute respiratory failure: a systematic review and meta-analysis of randomized controlled trials
- PMID: 29237436
- PMCID: PMC5729290
- DOI: 10.1186/s12890-017-0525-0
High-flow nasal cannula oxygen therapy versus conventional oxygen therapy in patients with acute respiratory failure: a systematic review and meta-analysis of randomized controlled trials
Abstract
Background: Acute respiratory failure (ARF) is a common and life-threatening medical emergency in patients admitted to the hospital. Currently, there is a lack of large-scale evidence on the use of high-flow nasal cannulas (HFNC) in patients with ARF. In this systematic review and meta-analysis, we evaluated whether there were differences between HFNC therapy and conventional oxygen therapy (COT) for treating patients with ARF.
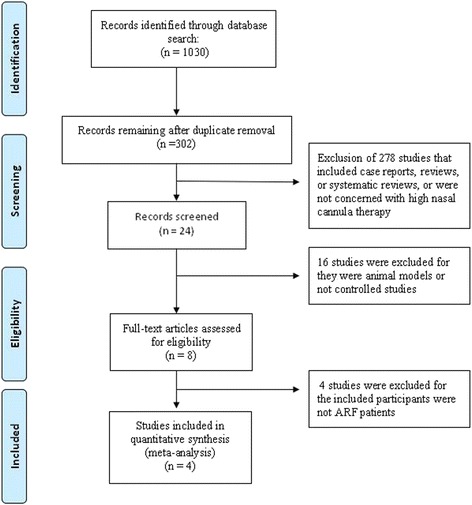
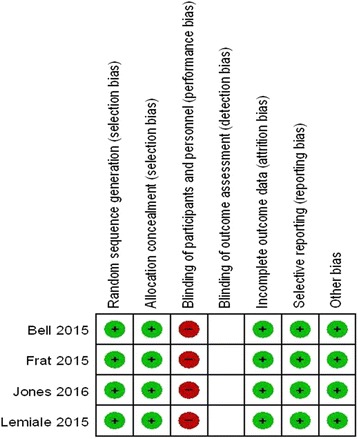
Methods: The EMBASE, Medline, and Wanfang databases and the Cochrane Library were searched. Two investigators independently collected the data and assessed the quality of each study. Randomized controlled trials that compared HFNC therapy with COT in patients with ARF were included. RevMan 5.3 was used to conduct the meta-analysis.
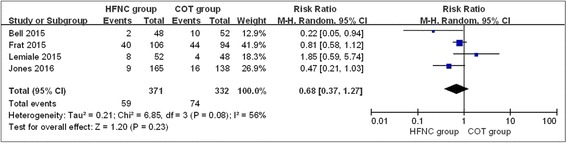
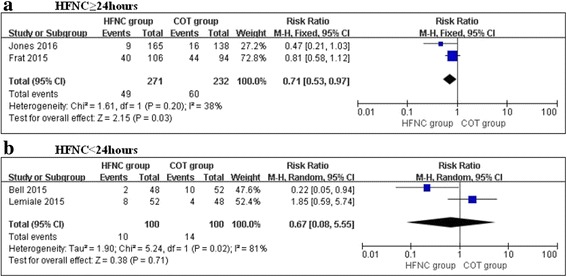
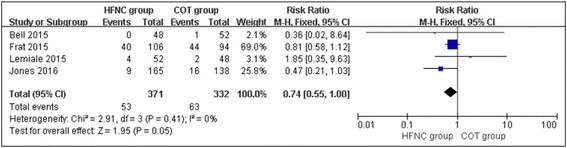
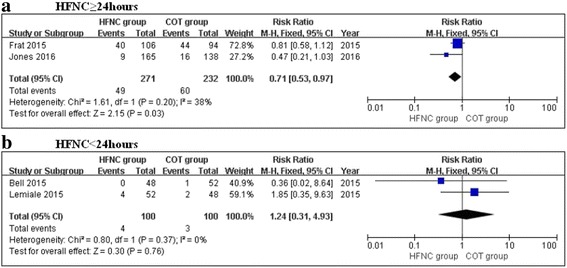
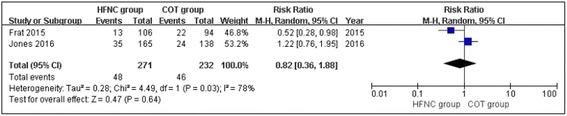
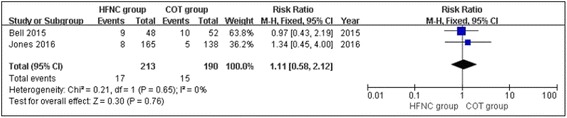
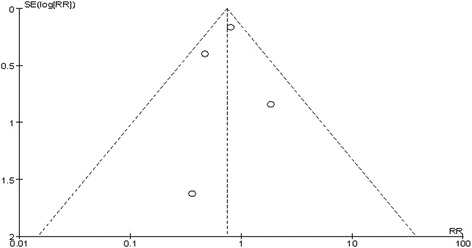
Results: Four studies that involved 703 patients with ARF were included, with 371 patients in the HFNC group and 332 patients in the COT group. In the overall estimates, there were no significant differences between the HFNC and COT groups in the rates of escalation of respiratory support (RR, 0.68; 95% CI, 0.37, 1.27; z = 1.20, P = 0.23), intubation (RR, 0.74; 95% CI, 0.55, 1.00; z = 1.95, P = 0.05), mortality (RR, 0.82; 95% CI, 0.36, 1.88; z = 0.47, P = 0.64), or ICU transfer (RR, 1.09; 95% CI, 0.57, 2.09; z = 0.26, P = 0.79) during ARF treatment. However, the subgroup analysis showed that HFNC therapy may decrease the rate of escalation of respiratory support (RR, 0.71; 95% CI, 0.53, 0.97; z = 2.15, P = 0.03) and the intubation rate (RR, 0.71; 95% CI, 0.53, 0.97; z = 2.15, P = 0.03) when ARF patients were treated with HFNC therapy for ≥24 h compared with COT.
Conclusions: HFNC therapy was similar to COT in ARF patients. The subgroup analysis showed that HFNC therapy may decrease the rate of escalation of respiratory support and the intubation rate when ARF patients were treated with HFNC for ≥24 h compared with COT. Further high-quality, large-scale studies are needed to confirm our results.
Keywords: Acute respiratory failure; High-flow nasal cannula; Mortality; Treatment.
Conflict of interest statement
Ethics approval and consent to participate
This is a meta-analysis, thus patient consent and ethical approval are not required.
Consent for publication
Not applicable.
Competing interests
The authors declare they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Bell N, Hutchinson CL, Green TC, Rogan E, Bein KJ, Dinh MM. Randomised control trial of humidified high flow nasal cannulae versus standard oxygen in the emergency department. Emerg Med Australas. 2015; 10.1111/1742-6723.12490. [Epub ahead of print] - PubMed
-
- Azoulay E, Mokart D, Pène F, et al. Outcomes of critically ill patients with hematologic malignancies: prospective multicenter data from France and Belgium—a Groupe de Recherche Respiratoire en reanimation Onco-Hématologique study. J Clin Oncol. 2013;31(22):2810–2818. doi: 10.1200/JCO.2012.47.2365. - DOI - PubMed
-
- Roca O, Riera J, Torres F, Masclans JR. High-flow oxygen therapy in acute respiratory failure. Respir Care. 2010;55(4):408–413. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
