

Left ventricular synchrony, torsion, and recoil mechanics in Ebstein's anomaly: insights from cardiovascular magnetic resonance
- PMID: 29237468
- PMCID: PMC5729283
- DOI: 10.1186/s12968-017-0414-y
Left ventricular synchrony, torsion, and recoil mechanics in Ebstein's anomaly: insights from cardiovascular magnetic resonance
Abstract
Background: Disease progression and heart failure development in Ebstein's Anomaly (EA) of the tricuspid valve is characterized by both right and left ventricular (LV) deterioration. The mechanisms underlying LV dysfunction and their role in heart failure development are incompletely understood. We hypothesized that LV dyssynchrony and impaired torsion and recoil mechanics induced by paradoxical movement of the basal septum may play a role in heart failure development.
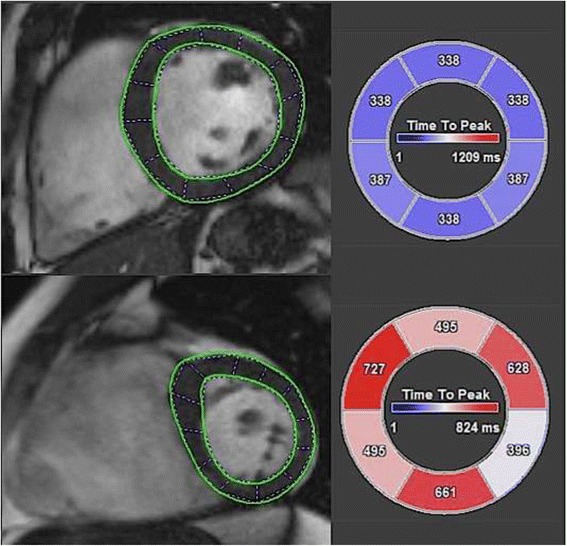
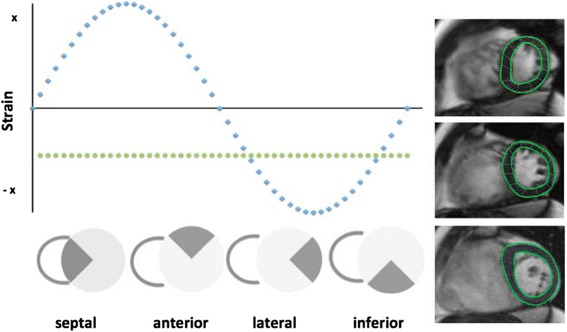
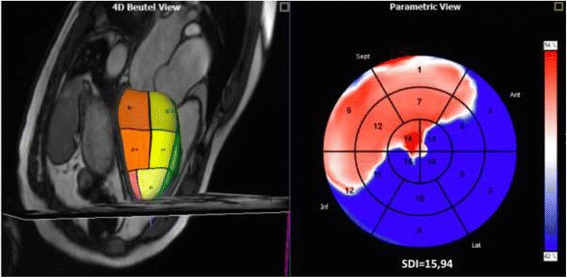
Methods: 31 EA patients and 31 matched controls underwent prospective cardiovascular magnetic resonance (CMR). CMR feature tracking (CMR-FT) was performed on apical, midventricular and basal short-axis and 4D-volume analysis was performed using three long-axis views and a short axis cine stack employing dedicated software. Circumferential uniformity ratio estimates (CURE) time-to-peak-based circumferential systolic dyssynchrony index (C-SDI), 4D volume analysis derived SDI (4D-SDI), torsion (Tor) and systolic (sysTR) and diastolic torsion rate (diasTR) were calculated for the LV. QRS duration, brain natriuretic peptide, NYHA and Total R/L-Volume Index (R/L Index) were obtained.
Results: EA patients (31.5 years; controls 31.4 years) had significantly longer QRS duration (123.35 ms ± 26.36 vs. 97.33 ms ± 11.89 p < 0.01) and showed more LV dyssynchrony (4D-SDI 7.60% ± 4.58 vs. 2.54% ± 0.62, p < 0.001; CURE 0.77 ± 0.05 vs. 0.86 ± 0.03, p < 0.001; C-SDI 7.70 ± 3.38 vs. 3.80 ± 0.91, p = 0.001). There were significant associations of LV dyssynchrony with heart failure parameters and QRS duration. Although torsion and recoil mechanics did not differ significantly (p > 0.05) there was an association of torsion and recoil mechanics with dyssynchrony parameters CURE (sysTR r = -0.426; p = 0.017, diasTR r = 0.419; p = 0.019), 4D-SDI (sysTR r = 0.383; p = 0.044) and C-SDI (diasTR r = -0.364; p = 0.044).
Conclusions: EA is characterized by LV intra-ventricular dyssynchrony, which is associated with heart failure and disease severity parameters. Markers of dyssynchrony can easily be quantified from CMR-FT, and may have a role in the assessment of altered cardiac function, carrying potential management implications for EA patients.
Keywords: CMR feature tracking; Congenital heart disease; Dyssynchrony; Ebstein anomaly; Heart failure; Left ventricle; Torsion and recoil.
Conflict of interest statement
Ethics approval and consent to participate
The study was approved by the Ethics Committee of the University Medical Center, Georg-August-University Göttingen, Germany and complies with the declaration of Helsinki and its amendments. Written informed consent was obtained from all participants.
Consent for publication
All authors have read and approved the final version of the manuscript and have consented to submission in its present form
Competing interests
None of the authors has competing interests to report.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Hosch O, Ngyuen TT, Lauerer P, Schuster A, Kutty S, Staab W, Unterberg-Buchwald C, Sohns JM, Paul T, Lotz J, Steinmetz M. BNP and haematological parameters are markers of severity of Ebstein’s anomaly: correlation with CMR and cardiopulmonary exercise testing. European heart journal cardiovascular Imaging. 2015;16:670–675. - PubMed
-
- Taylor RJ, Umar F, Moody WE, Meyyappan C, Stegemann B, Townend JN, Hor KN, Miszalski-Jamka T, Mazur W, Steeds RP, Leyva F. Feature-tracking cardiovascular magnetic resonance as a novel technique for the assessment of mechanical dyssynchrony. Int J Cardiol. 2014;175:120–125. doi: 10.1016/j.ijcard.2014.04.268. - DOI - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
