

Patient characteristics, resource use and outcomes associated with general internal medicine hospital care: the General Medicine Inpatient Initiative (GEMINI) retrospective cohort study
- PMID: 29237706
- PMCID: PMC5741428
- DOI: 10.9778/cmajo.20170097
Patient characteristics, resource use and outcomes associated with general internal medicine hospital care: the General Medicine Inpatient Initiative (GEMINI) retrospective cohort study
Abstract
Background: The precise scope of hospital care delivered under general internal medicine services remains poorly quantified. The purpose of this study was to describe the demographic characteristics, medical conditions, health outcomes and resource use of patients admitted to general internal medicine at 7 hospital sites in the Greater Toronto Area.
Methods: This was a retrospective cohort study involving all patients who were admitted to or discharged from general internal medicine at the study sites between Apr. 1, 2010, and Mar. 31, 2015. Clinical data from hospital electronic information systems were linked to administrative data from each hospital. We examined trends in resource use and patient characteristics over the study period.
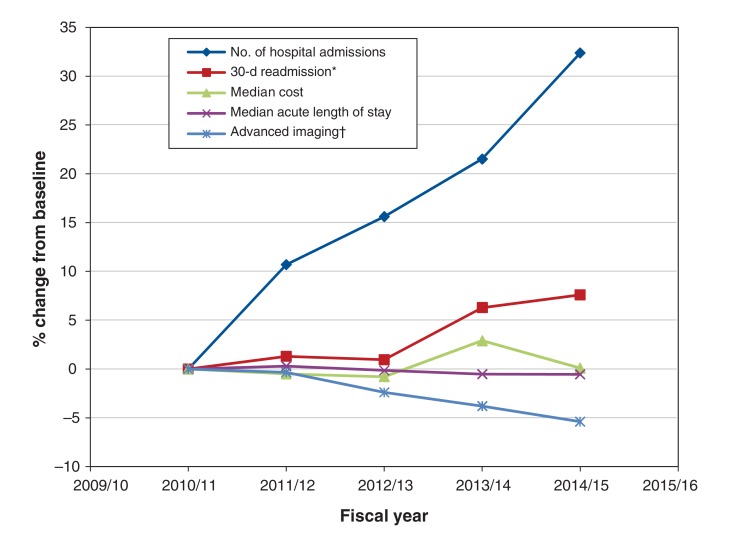
Results: There were 136 208 admissions to general internal medicine involving 88 121 unique patients over the study period. General internal medicine admissions accounted for 38.8% of all admissions from the emergency department and 23.7% of all hospital bed-days. Over the study period, the number of admissions to general internal medicine increased by 32.4%; there was no meaningful change in the median length of stay or cost per hospital stay. The median patient age was 73 (interquartile range [IQR] 57-84) years, and the median number of coexisting conditions was 6 (IQR 3-9). The median acute length of stay was 4.6 (IQR 2.5-8.6) days, and the median total cost per hospital stay was $5850 (IQR $3915-$10 061). Patients received at least 1 computed tomography scan in 52.2% of admissions. The most common primary discharge diagnoses were pneumonia (5.0% of admissions), heart failure (4.7%), chronic obstructive pulmonary disease (4.1%), urinary tract infection (4.0%) and stroke (3.6%).
Interpretation: Patients admitted to general internal medicine services represent a large, heterogeneous, resource-intensive and growing population. Understanding and improving general internal medicine care is essential to promote a high-quality, sustainable health care system.
Copyright 2017, Joule Inc. or its licensors.
Conflict of interest statement
Competing interests: Muhammad Mamdani has served on the advisory boards of and reports personal fees from Bristol-Myers Squibb, Eli Lilly and Company, GlaxoSmithKline, Hoffman-La Roche, Novartis, Novo Nordisk, Pfizer and AstraZeneca outside of the submitted work. Irfan Dhalla is Vice-president of Evidence Development and Standards at Health Quality Ontario. Any opinions or conclusions expressed in this publication do not necessarily represent the opinions or conclusions of Health Quality Ontario. No endorsement is intended or should be inferred.
Figures
References
-
- National health expenditure trends, 1975 to 2016. Ottawa: Canadian Institute for Health Information; 2016.
-
- Soong C, Fan E, Howell EE, et al. Characteristics of hospitalists and hospitalist programs in the United States and Canada. J Clin Outcomes Manag. 2009;16:69–74.
-
- Uijen AA, van de Lisdonk EH. Multimorbidity in primary care: prevalence and trend over the last 20 years. Eur J Gen Pract. 2008;14:28–32. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous