

Rationale and Descriptive Analysis of Specific Health Guidance: the Nationwide Lifestyle Intervention Program Targeting Metabolic Syndrome in Japan
- PMID: 29238010
- PMCID: PMC5906184
- DOI: 10.5551/jat.42010
Rationale and Descriptive Analysis of Specific Health Guidance: the Nationwide Lifestyle Intervention Program Targeting Metabolic Syndrome in Japan
Abstract
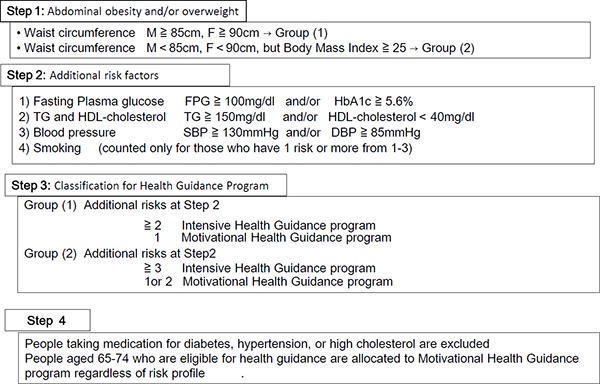
Aim: All health insurers in Japan are mandated to provide Specific Health Checkups and Specific Health Guidance (SHG) focusing on metabolic syndrome (MetS) in middle-aged adults, beginning in 2008; intensive HG for individuals who have abdominal obesity and two or more additional MetS risk factors, and motivational HG for individuals with one risk factor. The aim of this study is to describe medium-term changes in health indexes for intensive and motivational HG groups using the National Database.
Methods: We compared changes of risk factors and initiation of pharmacological therapy over 3 yr between participants (n=31,790) and nonparticipants (n=189,726) who were eligible for SHG in 2008.
Results: Body weight reduction in intensive HG was 1.98 kg (participants) vs 0.42 kg (nonparticipants) in men (p<0.01) and 2.25 vs 0.68 kg in women (p<0.01) after 1 yr. In motivational HG, the respective reduction was 1.40 vs 0.30 kg in men (p<0.01) and 1.53 vs 0.42 kg in women (p<0.01). Waist circumference reduction was also greatest among participants in intensive HG (2.34 cm in men and 2.98 cm in women). These reductions were fairly unchanged over 3 yr and accompanied greater improvements in MetS risk factors in participants. We also detected significantly smaller percentages of SHG participants who initiated pharmacological therapy compared with nonparticipants.
Conclusion: Participants in SHG showed greater improvements in MetS profiles with proportionally smaller pharmacological treatment initiations than did nonparticipants for 3 yr. Although selection bias may be present, this study suggests SHG would be a feasible strategy to prevent MetS and its sequelae.
Keywords: Health Guidance; Health Policy; Health checkup; Metabolic Syndrome; National Data Base.
Conflict of interest statement
ALL authors have nothing to disclose.
Figures



Comment in
-
Specific Health Guidance, the Nationwide Lifestyle Intervention Program Targeting Metabolic Syndrome, Seems to be Successful in Japan.J Atheroscler Thromb. 2018 Apr 1;25(4):304-305. doi: 10.5551/jat.ED092. Epub 2018 Feb 22. J Atheroscler Thromb. 2018. PMID: 29467342 Free PMC article. No abstract available.
References
-
- OECD Data : Life Expectancy at Birth. Organization for Economic Co-operation and Development, Paris: https://data.oecd.org/healthstat/life-expectancy-at-birth.htm
-
- Ikeda N, Saito E, Kondo N, Inoue M, Ikeda S, Satoh T, Wada K, Stickley A, Katanoda K, Mizoue T, Noda M, Iso H, Fujino Y, Sobue T, Tsugane S, Naghavi M, Ezzati M, Shibuya K. What has made the population of Japan healthy? Lancet 2011; 378: 1094-1105 - PubMed
-
- Johansson SR, Mosk C. Exposure, resistance and life expectancy: disease and death during the economic development of Japan, 1900–1960. Pupul Stud (Camb) 1987; 41: 207-235 - PubMed
-
- Ikegami N, Yoo BK, Hashimoto H, Matsumoto M, Ogata H, Babazono A, Watanabe R, Shibuya K, Yang BM, Reich MR, Kobayashi Y. Japanese universal health coverage: evolution, achievements, and challenges. Lancet 2011; 378: 1106-1115 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical