

Clinicians approaches to management of background treatment in patients with SLE in clinical remission: results of an international observational survey
- PMID: 29238601
- PMCID: PMC5724341
- DOI: 10.1136/lupus-2016-000173
Clinicians approaches to management of background treatment in patients with SLE in clinical remission: results of an international observational survey
Abstract
Background: The definition of remission in systemic lupus erythematosus (SLE) remains unclear, especially how background treatment should be interpreted.
Objective: To determine preferences of clinicians in treatment of patients in clinical remission from SLE and to assess how previous severity, duration of remission and serology influence changes in treatment.
Methods: We undertook an internet-based survey of clinicians managing patients with SLE. Case scenarios were constructed to reflect different remission states, previous organ involvement, serological abnormalities, duration of remission and current treatment (hydroxychloroquine (HCQ), steroids and/or immunosuppressive (ISS) agents).
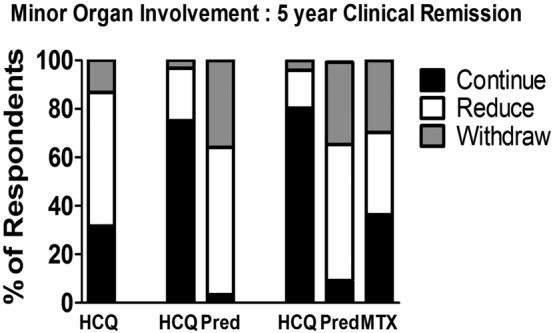
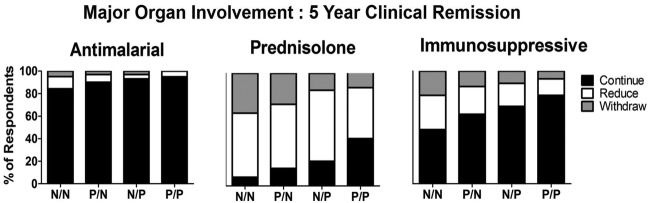
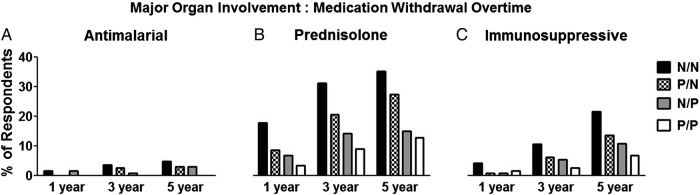
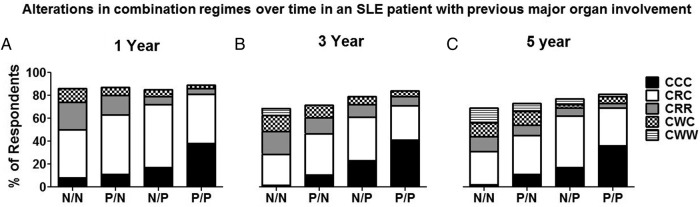
Results: 130 clinicians from 30 countries were surveyed. The median (range) duration of practice and number of patients with SLE seen each month was 13 (2-42) years and 30 (2-200), respectively. Management decisions in all scenarios varied with greater caution in treatment reduction with shorter duration of remission, extent of serological abnormalities and previous disease severity. Even with mild disease, normal serology and a 5-year clinical remission, 113 (86.9%) clinicians continue to prescribe HCQ. Persistent abnormal serology in any scenario led to a reluctance to reduce or discontinue medications. Prescribing in remission, particularly of steroids and HCQ, varied significantly according to geographical location.
Conclusions: Clinicians preferences in withdrawing or reducing treatment in patients with SLE in clinical remission vary considerably. Serological abnormalities, previous disease severity and duration of remission all influence the decision to reduce treatment. It is unusual for clinicians to stop HCQ even after prolonged periods of clinical remission. Any definition(s) of remission needs to take into consideration such evidence on how maintenance treatments are managed.
Keywords: Corticosteroids; Disease Activity; Remission; Systemic Lupus Erythematosus; serology.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- Rahman A, Isenberg DA. Systemic lupus erythematosus. N Engl J Med 2008;358:929–39. doi:10.1056/NEJMra071297 - DOI - PubMed
-
- Cervera R, Khamashta MA, Font J, et al. Morbidity and mortality in systemic lupus erythematosus during a 10-year period: a comparison of early and late manifestations in a cohort of 1,000 patients. Medicine (Baltimore) 2003;82:299–308. doi:10.1097/01.md.0000091181.93122.55 - DOI - PubMed
-
- Urowitz MB, Feletar M, Bruce IN, et al. Prolonged remission in systemic lupus erythematosus. J Rheumatol 2005;32:1467–72. - PubMed
-
- Ruperto N, Hanrahan LM, Alarcón GS, et al. International consensus for a definition of disease flare in lupus. Lupus 2011;20:453–62. doi:10.1177/0961203310388445 - DOI - PubMed
-
- van Vollenhoven RF, Mosca M, Bertsias G, et al. Treat-to-target in systemic lupus erythematosus: recommendations from an international task force. Ann Rheum Dis 2014;73:958–67. doi:10.1136/annrheumdis-2013-205139 - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources