

Flexible Laryngoscopy in Management of Congenital Stridor
- PMID: 29238683
- PMCID: PMC5714909
- DOI: 10.1007/s12070-017-1217-z
Flexible Laryngoscopy in Management of Congenital Stridor
Abstract
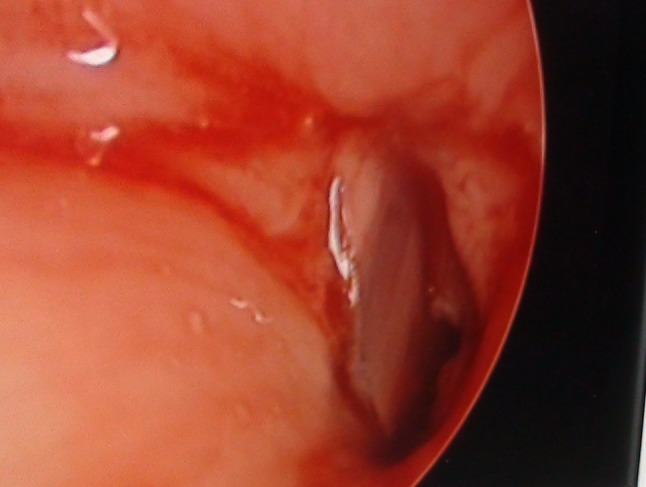
The incidence of congenital stridor is on rise due to improved neonate and infant survival rate. The gold standard investigation for evaluation of stridor is rigid laryngotracheobronchoscopy, but this is invasive and requires general anesthesia. Flexible fibreoptic laryngoscopy, a relatively simple and less invasive procedure can be done under topical anaesthesia for evaluation of stridor. In this study, we have presented our experience of flexible laryngoscopy in children with congenital stridor, their results and management. Laryngomalacia was the commonest cause of stridor accounting for 80% of cases. 15% (6) patients required tracheostomy for relieving airway obstruction and 22.5% (9) patients required a definitive surgical procedure for correcting the cause. Flexible laryngoscopy is safe and gives a comprehensive analysis of airway including its dynamic functions. We also recommend flexible laryngoscopy as a frontline investigation for evaluation of stridor.
Keywords: Congenital lesions; Flexible laryngoscopy; Stridor.
Conflict of interest statement
Compliance with Ethical StandardsThere were no conflict of interests between authors or anyone who participated in the study.Informed consent was obtained from the guardians/parents before performing the procedure.The procedures performed in the study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Figures




References
LinkOut - more resources
Full Text Sources
Other Literature Sources