

Estimated clinical impact of the Xpert MTB/RIF Ultra cartridge for diagnosis of pulmonary tuberculosis: A modeling study
- PMID: 29240766
- PMCID: PMC5730108
- DOI: 10.1371/journal.pmed.1002472
Estimated clinical impact of the Xpert MTB/RIF Ultra cartridge for diagnosis of pulmonary tuberculosis: A modeling study
Abstract
Background: The Xpert MTB/RIF (Xpert) assay offers rapid and accurate diagnosis of tuberculosis (TB) but still suffers from imperfect sensitivity. The newer Xpert MTB/RIF Ultra cartridge has shown improved sensitivity in recent field trials, but at the expense of reduced specificity. The clinical implications of switching from the existing Xpert cartridge to the Xpert Ultra cartridge in different populations remain uncertain.
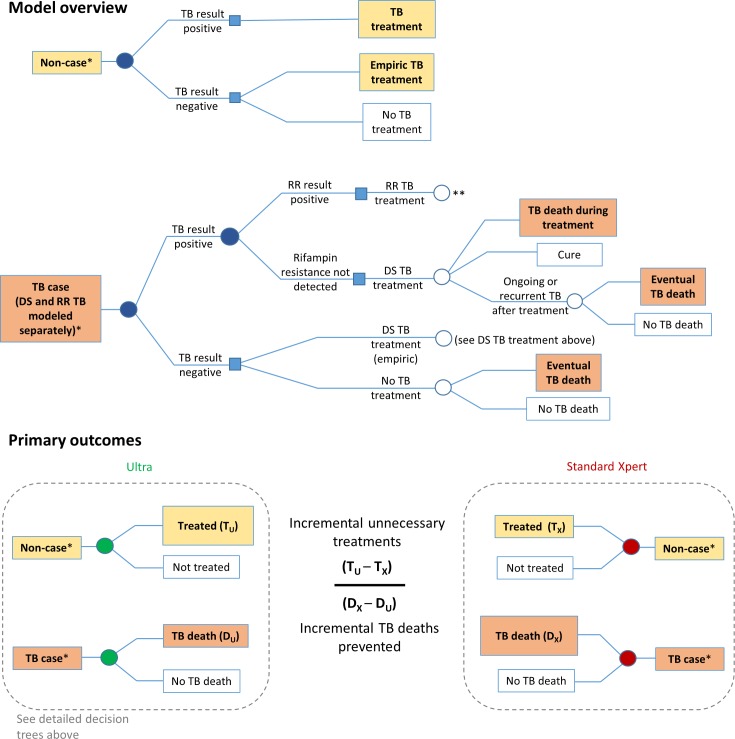
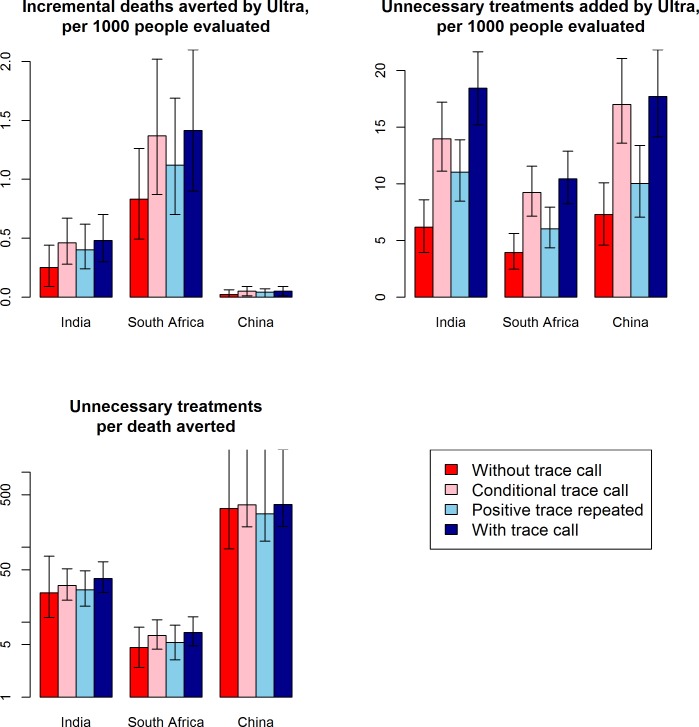
Methods and findings: We developed a Markov microsimulation model of hypothetical cohorts of 100,000 individuals undergoing diagnostic sputum evaluation with Xpert for suspected pulmonary TB, in each of 3 emblematic settings: an HIV clinic in South Africa, a public TB center in India, and an adult primary care setting in China. In each setting, we used existing data to project likely diagnostic results, treatment decisions, and ultimate clinical outcomes, assuming use of the standard Xpert versus Xpert Ultra cartridge. Our primary outcomes were the projected number of additional unnecessary treatments generated, the projected number of TB deaths averted, and the projected number of unnecessary treatments generated per TB death averted, if standard Xpert were switched to Xpert Ultra. We also simulated alternative approaches to interpreting positive results of the Ultra cartridge's semi-quantitative trace call. Extensive sensitivity and uncertainty analyses were performed to evaluate the drivers and generalizability of projected results. In the Indian TB center setting, replacing the standard Xpert cartridge with the Xpert Ultra cartridge was projected to avert 0.5 TB deaths (95% uncertainty range [UR]: 0, 1.3) and generate 18 unnecessary treatments (95% UR: 10, 29) per 1,000 individuals evaluated-resulting in a median ratio of 38 incremental unnecessary treatments added by Ultra per incremental death averted by Ultra compared to outcomes using standard Xpert (95% UR: 12, indefinite upper bound). In the South African HIV care setting-where TB mortality rates are higher and Ultra's improved sensitivity has greater absolute benefit-this ratio improved to 7 unnecessary treatments per TB death averted (95% UR: 2, 43). By contrast, in the Chinese primary care setting, this ratio was much less favorable, at 372 unnecessary treatments per TB death averted (95% UR: 75, indefinite upper bound), although the projected number of unnecessary treatments using Xpert Ultra was lower (with a possibility of no increased overtreatment) when using specificity data only from lower-burden settings. Alternative interpretations of the trace call had little effect on these ratios. Limitations include uncertainty in key parameters (including the clinical implications of false-negative results), the exclusion of transmission effects, and restriction of this analysis to adult pulmonary TB.
Conclusions: Switching from the standard Xpert cartridge to the Xpert Ultra cartridge for diagnosis of adult pulmonary TB may have different consequences in different clinical settings. In settings with high TB and HIV prevalence, Xpert Ultra is likely to offer considerable mortality benefit, whereas in lower-prevalence settings, Xpert Ultra will likely result in considerable overtreatment unless the possibility of higher specificity of Ultra in lower-prevalence settings in confirmed. The ideal use of the Ultra cartridge may therefore involve a more nuanced, setting-specific approach to implementation, with priority given to populations in which the anticipated prevalence of TB (and HIV) is the highest.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Boehme CC, Nicol MP, Nabeta P, Michael JS, Gotuzzo E, Tahirli R, et al. Feasibility, diagnostic accuracy, and effectiveness of decentralised use of the Xpert MTB/RIF test for diagnosis of tuberculosis and multidrug resistance: a multicentre implementation study. Lancet. 2011;377(9776):1495–505. doi: 10.1016/S0140-6736(11)60438-8 - DOI - PMC - PubMed
-
- Steingart KR, Schiller I, Horne DJ, Pai M, Boehme CC, Dendukuri N. Xpert® MTB/RIF assay for pulmonary tuberculosis and rifampicin resistance in adults. Cochrane Database Syst Rev. 2014;(1):CD009593 doi: 10.1002/14651858.CD009593.pub3 - DOI - PMC - PubMed
-
- Lawn SD, Mwaba P, Bates M, Piatek A, Alexander H, Marais BJ, et al. Advances in tuberculosis diagnostics: the Xpert MTB/RIF assay and future prospects for a point-of-care test. Lancet Infect Dis. 2013;13(4):349–61. doi: 10.1016/S1473-3099(13)70008-2 - DOI - PMC - PubMed
-
- Alland D, Rowneki M, Smith L, Ryan J, Chancellor M, Simmons AM, et al. Xpert MTB/RIF Ultra: a new near-patient TB test with sensitivity equal to culture. Conference on Retroviruses and Opportunistic Infections; 2015. February 23–26; Seattle, WA, US.
-
- Dorman SE, Schumacher SG, Alland D, Nabeta P, Armstrong DT, King B, et al. Xpert MTB/RIF Ultra for detection of Mycobacterium tuberculosis and rifampin resistance: a multicentre diagnostic accuracy study. Lancet Infect Dis [Internet]. 2017. November 30 [cited 2017 Dec 1]. Available from: http://dx.doi.org/10.1016/S1473-3099(17)30691-6. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
