

Review
doi: 10.1016/j.jpeds.2017.10.031.
Epub 2017 Dec 11.
Language Dysfunction in Pediatric Epilepsy
Affiliations
- PMID: 29241678
- PMCID: PMC5826845
- DOI: 10.1016/j.jpeds.2017.10.031
Item in Clipboard
Review
Language Dysfunction in Pediatric Epilepsy
J Pediatr.
2018 Mar.
No abstract available
Keywords: Landau-Kleffner syndrome; acquired language disorders; epilepsy; epilepsy surgery; epilepsy, rolandic; functional neuroimaging; language; language development; status epilepticus, electrographic.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
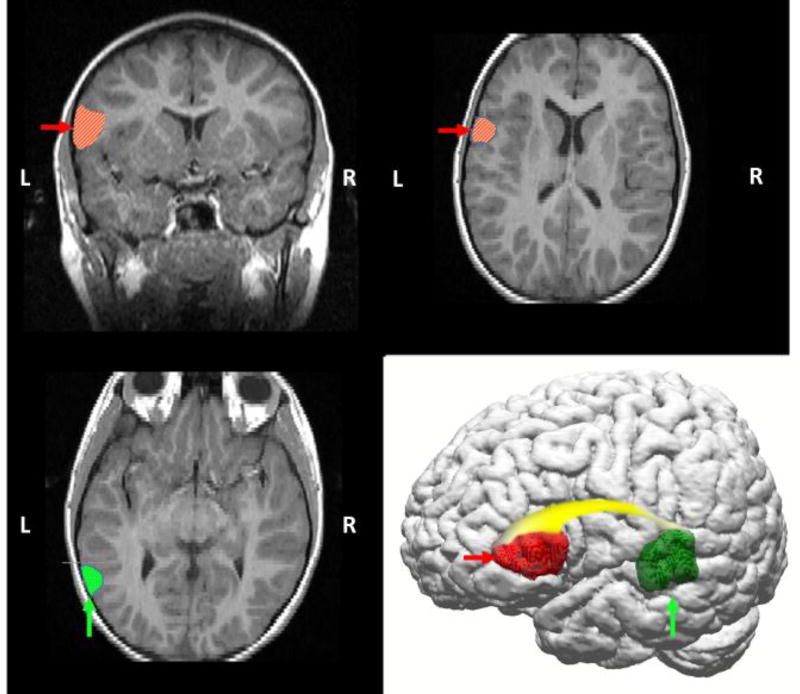
Diagrammatic representation of primary language areas on anatomical T2-weighted FLAIR MRI and 3D reconstruction images (110), highlighting left temporal lobe (Wernicke’s area in posterior temporal region, vertical arrows/dotted hatching), frontal lobe (Broca’s area in middle frontal region, horizontal arrows/diagonal hatching), and the white matter (arcuate fasciculus, gradient shading) that connects these regions. Historically, language has been conceptualized as a lateralized function, with dominance typically in the left hemisphere. Functional magnetic resonance imaging (fMRI) studies confirm that language is a left-hemispheric dominant process in the vast majority of healthy adults (111), but also that language requires input from distributed networks, including homologous right hemispheric regions.
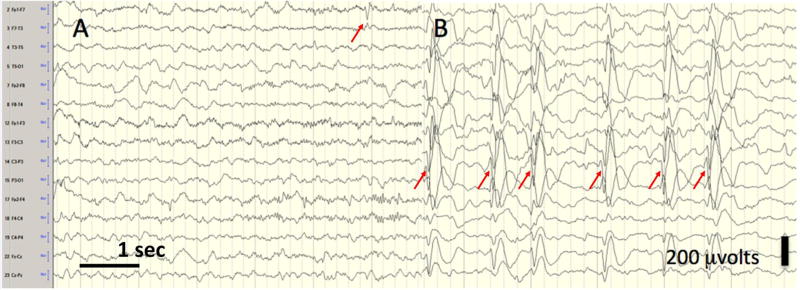
Electrical Status Epilepticus of Sleep (ESES). The EEG of a young girl with language regression; six seconds each of wakefulness (left panel, A) and slow wave sleep (right panel, B). In sleep, the EEG is similar in appearance to that seen in clinical status epilepticus (bipolor longitudinal montage; 10 uvolts/mm, low filter 0.1 Hz, high filter 70 Hz). In ESES, spikes are typically bitemporal, but may be lateralized, and sleep architecture is interrupted if present. Here, arrows indicate left tempo-parietal spikes with a field to the right hemisphere. When an EEG is evaluated for ESES, the percentage of seconds of non-REM sleep containing spikes is determined, with the cut-off for diagnosis varying between 50–85%.(16)
References
-
- Berg AT, Jallon P, Preux PM. The epidemiology of seizure disorders in infancy and childhood: definitions and classifications. Handb Clin Neurol. 2013;111:391–8. - PubMed
-
- Oka E, Ohtsuka Y, Yoshinaga H, Murakami N, Kobayashi K, Ogino T. Prevalence of childhood epilepsy and distribution of epileptic syndromes: a population-based survey in Okayama, Japan. Epilepsia. 2006;47:626–30. - PubMed
-
- Nickels KC, Zaccariello MJ, Hamiwka LD, Wirrell EC. Cognitive and neurodevelopmental comorbidities in paediatric epilepsy. Nat Rev Neurol. 2016;12:465–76. - PubMed
-
- Ferro MA, Camfield CS, Levin SD, Smith ML, Wiebe S, Zou G, et al. Trajectories of health-related quality of life in children with epilepsy: a cohort study. Epilepsia. 2013;54:1889–97. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
