

Second Arterial Versus Venous Conduits for Multivessel Coronary Artery Bypass Surgery in California
- PMID: 29242351
- PMCID: PMC9856244
- DOI: 10.1161/CIRCULATIONAHA.117.030959
Second Arterial Versus Venous Conduits for Multivessel Coronary Artery Bypass Surgery in California
Abstract
Background: Whether a second arterial conduit improves outcomes after multivessel coronary artery bypass grafting remains unclear. Consequently, arterial conduits other than the left internal thoracic artery are seldom used in the United States.
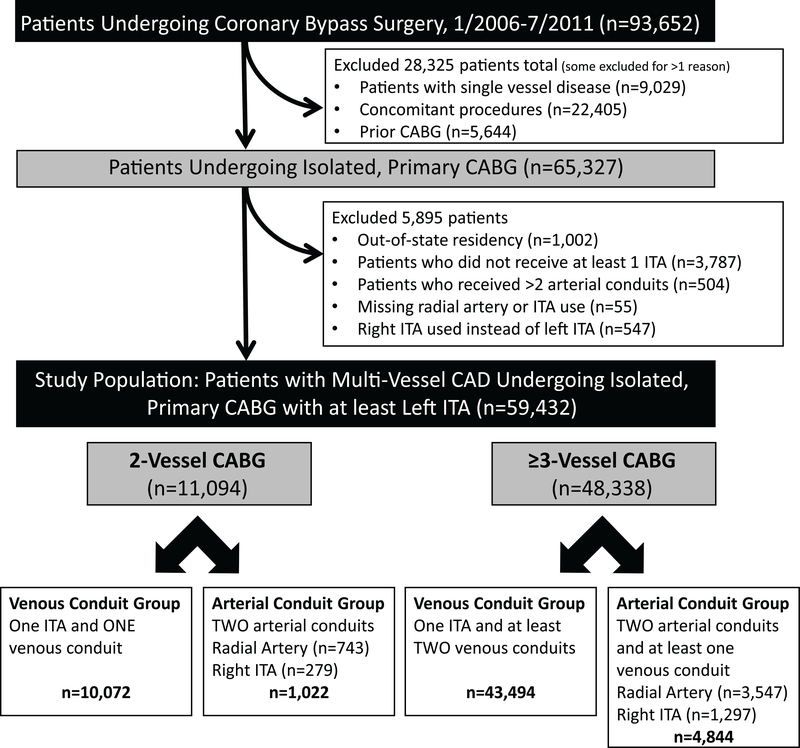
Methods: Using a state-maintained clinical registry including all 126 nonfederal hospitals in California, we compared all-cause mortality and rates of stroke, myocardial infarction, repeat revascularization, and sternal wound infection between propensity score-matched cohorts who underwent primary, isolated multivessel coronary artery bypass grafting with the left internal thoracic artery, and who received a second arterial conduit (right internal thoracic artery or radial artery, n=5866) or a venous conduit (n=53 566) between 2006 and 2011. Propensity score matching using 34 preoperative characteristics yielded 5813 matched sets. A subgroup analysis compared outcomes between propensity score-matched recipients of a right internal thoracic artery (n=1576) or a radial artery (n=4290).
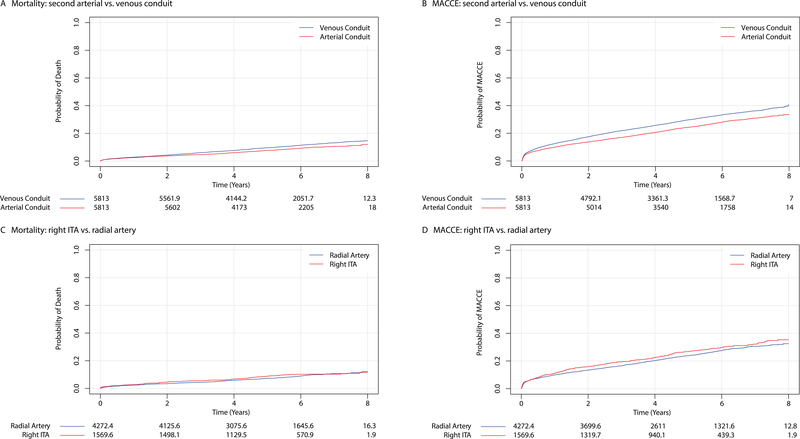
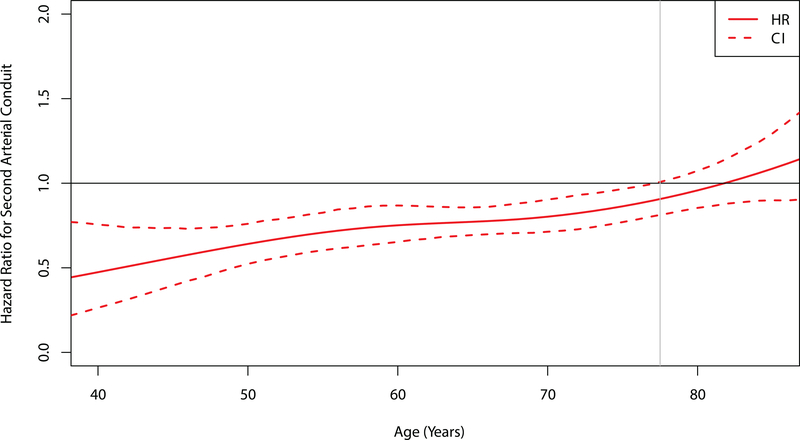
Results: Second arterial conduit use decreased from 10.7% in 2006 to 9.1% in 2011 (P<0.0001). However, receipt of a second arterial conduit was associated with significantly lower mortality (13.1% versus 10.6% at 7 years; hazard ratio, 0.79; 95% confidence interval [CI], 0.72-0.87), and lower risks of myocardial infarction (hazard ratio, 0.78; 95% CI, 0.70-0.87) and repeat revascularization (hazard ratio, 0.82; 95% CI, 0.76-0.88). In comparison with radial artery grafts, right internal thoracic artery grafts were associated with similar mortality rates (right internal thoracic artery 10.3% versus radial artery 10.7% at 7 years; hazard ratio, 1.10; 95% CI, 0.89-1.37) and individual risks of cardiovascular events, but the risk of sternal wound infection was increased (risk difference, 1.07%; 95% CI, 0.15-2.07).
Conclusions: Second arterial conduit use in California is low and declining, but arterial grafts were associated with significantly lower mortality and fewer cardiovascular events. A right internal thoracic artery graft offered no benefit over that of a radial artery, but did increase risk of sternal wound infection. These findings suggest surgeons should consider lowering their threshold for using arterial grafts, and the radial artery may be the preferred second conduit.
Keywords: coronary artery bypass; internal thoracic artery; propensity score; radial artery.
© 2017 American Heart Association, Inc.
Figures
Comment in
-
Why Don't We Kill 2 Birds with 1 Stone? Less Adverse Cardiac Events and Improved Survival With Multiarterial Coronary Artery Bypass Grafting.Circulation. 2018 Apr 17;137(16):1708-1711. doi: 10.1161/CIRCULATIONAHA.117.032885. Circulation. 2018. PMID: 29661950 No abstract available.
References
-
- Benjamin EJ, Blaha MJ, Chiuve SE, Cushman M, Das SR, Deo R, de Ferranti SD, Floyd J, Fornage M, Gillespie C, Isasi CR, Jimenez MC, Jordan LC, Judd SE, Lackland D, Lichtman JH, Lisabeth L, Liu S, Longenecker CT, Mackey RH, Matsushita K, Mozaffarian D, Mussolino ME, Nasir K, Neumar RW, Palaniappan L, Pandey DK, Thiagarajan RR, Reeves MJ, Ritchey M, Rodriguez CJ, Roth GA, Rosamond WD, Sasson C, Towfighi A, Tsao CW, Turner MB, Virani SS, Voeks JH, Willey JZ, Wilkins JT, Wu JH, Alger HM, Wong SS, Muntner P, American Heart Association Statistics C and Stroke Statistics S. Heart Disease and Stroke Statistics-2017 Update: A Report From the American Heart Association. Circulation. 2017;135:e146–e603. - PMC - PubMed
-
- European Heart Network. European Cardiovascular Disease Statistics 2017. http://www.ehnheart.org/cvd-statistics.html. Accessed October 21, 2017.
-
- Mohr FW, Morice MC, Kappetein AP, Feldman TE, Stahle E, Colombo A, Mack MJ, Holmes DR Jr., Morel MA, Van Dyck N, Houle VM, Dawkins KD and Serruys PW. Coronary artery bypass graft surgery versus percutaneous coronary intervention in patients with three-vessel disease and left main coronary disease: 5-year follow-up of the randomised, clinical SYNTAX trial. Lancet. 2013;381:629–638. - PubMed
-
- Farkouh ME, Domanski M, Sleeper LA, Siami FS, Dangas G, Mack M, Yang M, Cohen DJ, Rosenberg Y, Solomon SD, Desai AS, Gersh BJ, Magnuson EA, Lansky A, Boineau R, Weinberger J, Ramanathan K, Sousa JE, Rankin J, Bhargava B, Buse J, Hueb W, Smith CR, Muratov V, Bansilal S, King S 3rd, Bertrand M, Fuster V and Investigators FT. Strategies for multivessel revascularization in patients with diabetes. N Engl J Med. 2012;367:2375–2384. - PubMed
-
- Stone GW, Sabik JF, Serruys PW, Simonton CA, Genereux P, Puskas J, Kandzari DE, Morice MC, Lembo N, Brown WM 3rd, Taggart DP, Banning A, Merkely B, Horkay F, Boonstra PW, van Boven AJ, Ungi I, Bogats G, Mansour S, Noiseux N, Sabate M, Pomar J, Hickey M, Gershlick A, Buszman P, Bochenek A, Schampaert E, Page P, Dressler O, Kosmidou I, Mehran R, Pocock SJ, Kappetein AP and Investigators ET. Everolimus-Eluting Stents or Bypass Surgery for Left Main Coronary Artery Disease. N Engl J Med. 2016;375:2223–2235. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
