

Gaining Mechanistic Insight Into Coproporphyrin I as Endogenous Biomarker for OATP1B-Mediated Drug-Drug Interactions Using Population Pharmacokinetic Modeling and Simulation
- PMID: 29243231
- PMCID: PMC6175062
- DOI: 10.1002/cpt.983
Gaining Mechanistic Insight Into Coproporphyrin I as Endogenous Biomarker for OATP1B-Mediated Drug-Drug Interactions Using Population Pharmacokinetic Modeling and Simulation
Abstract
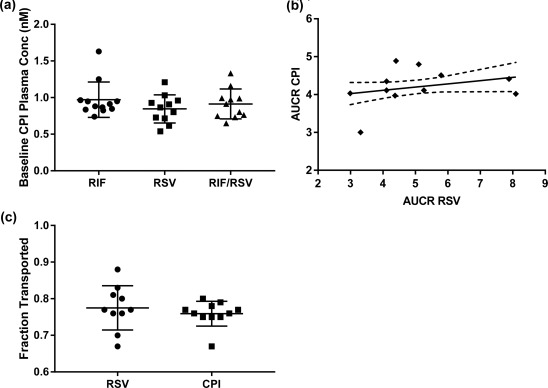
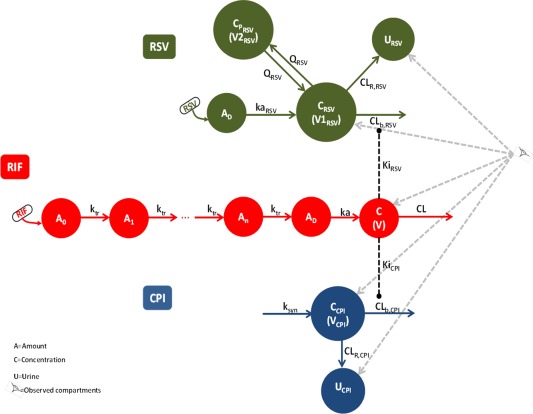
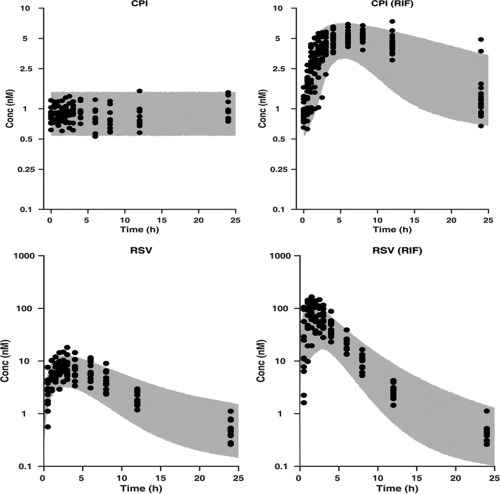
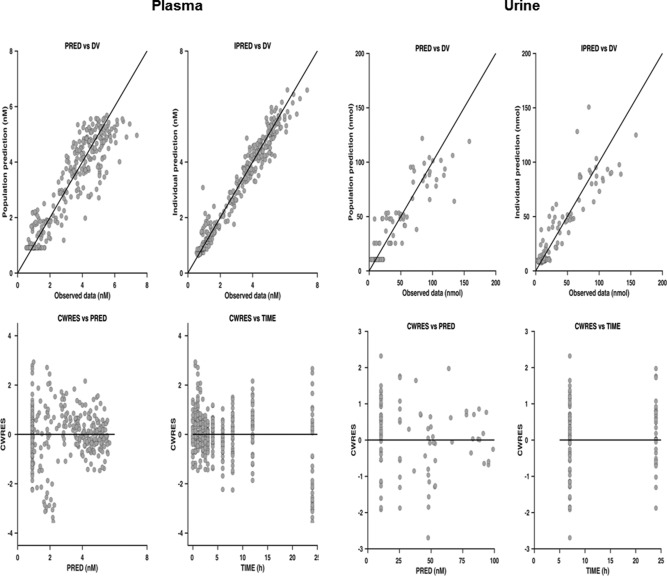
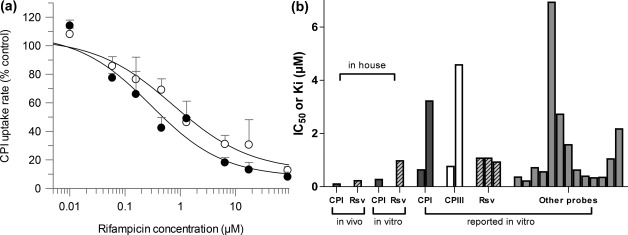
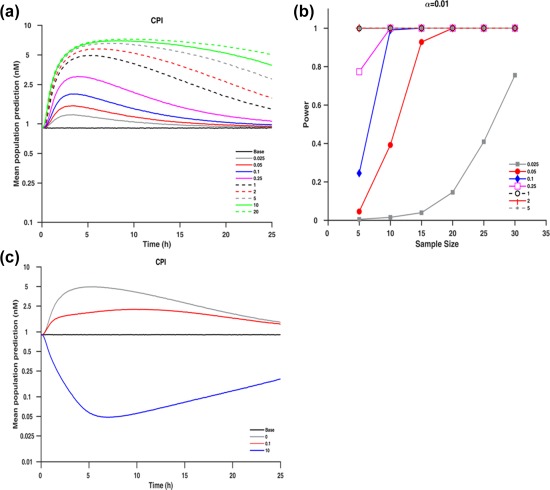
This study evaluated coproporphyrin I (CPI) as a selective endogenous biomarker of OATP1B-mediated drug-drug interactions (DDIs) relative to clinical probe rosuvastatin using nonlinear mixed-effect modeling. Plasma and urine CPI data in the presence/absence of rifampicin were modeled to describe CPI synthesis, elimination clearances, and obtain rifampicin in vivo OATP Ki. The biomarker showed stable interoccasion baseline concentrations and low interindividual variability (<25%) in subjects with wildtype SLCO1B1. Biliary excretion was the dominant CPI elimination route (maximal >85%). Estimated rifampicin in vivo unbound OATP Ki (0.13 μM) using CPI data was 2-fold lower relative to rosuvastatin. Model-based simulations and power calculations confirmed sensitivity of CPI to identify moderate and weak OATP1B inhibitors in an adequately powered clinical study. Current analysis provides the most detailed evaluation of CPI as an endogenous OATP1B biomarker to support optimal DDI study design; further pharmacogenomic and DDI data with a panel of inhibitors are required.
© 2017 The Authors Clinical Pharmacology & Therapeutics published by Wiley Periodicals, Inc. on behalf of American Society for Clinical Pharmacology and Therapeutics.
Figures
References
-
- Galetin, A. , Zhao, P. & Huang, S.M. Physiologically based pharmacokinetic modeling of drug transporters to facilitate individualized dose prediction. J. Pharm. Sci. 106, 2204–2208 (2017). - PubMed
-
- Rodrigues, A.D. , Taskar, K.S. , Kusuhara, H. & Sugiyama, Y. Endogenous probes for drug transporters: balancing vision with reality. Clin. Pharmacol. Ther. (2017) [Epub ahead of print]. - PubMed
-
- Yoshida, K. , Maeda, K. & Sugiyama, Y. Transporter‐mediated drug‐drug interactions involving OATP substrates: predictions based on in vitro inhibition studies. Clin. Pharmacol. Ther. 91, 1053–1064 (2012). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
