

Transient Myocardial Thickening in Cats Associated with Heart Failure
- PMID: 29243322
- PMCID: PMC5787177
- DOI: 10.1111/jvim.14897
Transient Myocardial Thickening in Cats Associated with Heart Failure
Abstract
Background: Cats with hypertrophic cardiomyopathy (HCM) and congestive heart failure (CHF) can have resolution of both left ventricular hypertrophy and CHF.
Objectives: To describe the clinical characteristics of cats with transient myocardial thickening (TMT) and CHF compared with a control population of cats without resolution of HCM.
Animals: A total of 21 cats with TMT, 21 cats with HCM.
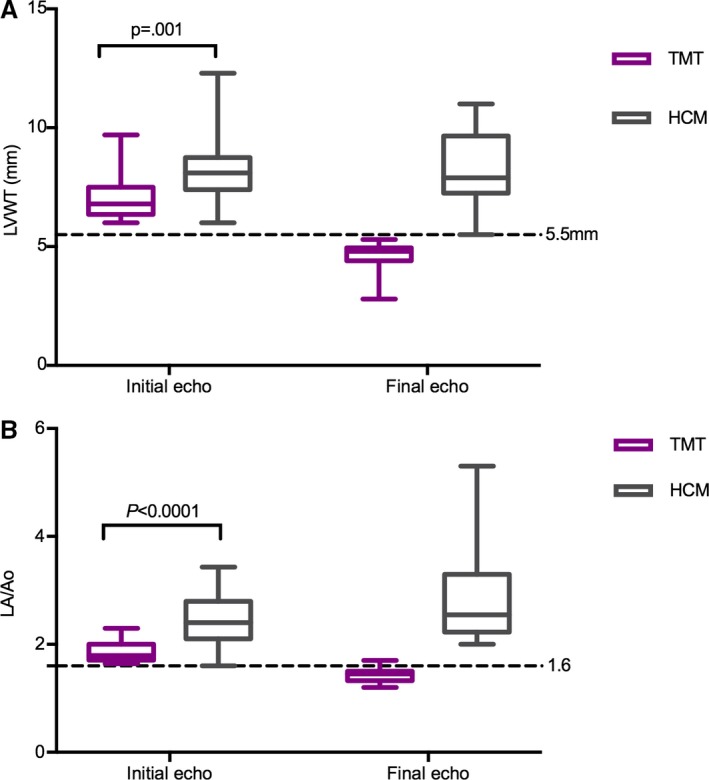
Methods: Retrospective study. Clinical records at 4 veterinary centers were searched for TMT cases and a control group of cats with HCM and CHF. TMT was defined as initial maximal left ventricular wall thickness (LVWT) ≥6 mm with left-sided CHF, with subsequent resolution of CHF, reduction in left atrium/aorta (LA/Ao), and LVWT<5.5 mm. HCM was defined as persistent LVWT ≥6 mm.
Results: Cats with TMT were younger (2 [0.4-11.4] years) than cats with HCM (8 [1.6-14] years) (P < 0.0001), and antecedent events were more common (15/21 versus 6/21, respectively) (P = 0.01). In cats with TMT, LVWT normalized from 6.8 [6.0-9.7] mm to 4.8 [2.8-5.3] mm and LA/Ao decreased from 1.8 [1.6-2.3] to 1.45 [1.2-1.7] after a mean interval of 3.3 (95% CI: 1.8-4.7) months. CHF recurred in 1 of 21 TMT and 15 of 21 cats with HCM. Cardiac treatment was discontinued in 20 of 21 cats with TMT and 0 of 21 HCM cats. All cats with TMT survived, whereas 8 of 19 cats with HCM died during the study period.
Conclusions and clinical importance: TMT occurs in younger cats, and antecedent events are common. The prognosis is better in cats with CHF associated with TMT than HCM.
Keywords: HCM phenocopy; Hypertrophic cardiomyopathy; Myocarditis; Takotsubo cardiomyopathy.
Copyright © 2017 The Authors. Journal of Veterinary Internal Medicine published by Wiley Periodicals, Inc. on behalf of the American College of Veterinary Internal Medicine.
Conflict of interest statement
Authors declare no conflict of interest.
Figures
References
-
- Elliott P, Andersson B, Arbustini E, et al. Classification of the cardiomyopathies: A position statement from the European Society Of Cardiology Working Group on Myocardial and Pericardial Diseases. Eur Heart J 2008;29:270–276. - PubMed
-
- Authors/Task Force members , Elliott PM, Anastasakis A, et al. 2014 ESC Guidelines on diagnosis and management of hypertrophic cardiomyopathy: The Task Force for the Diagnosis and Management of Hypertrophic Cardiomyopathy of the European Society of Cardiology (ESC). Eur Heart J 2014;35:2733–2779. - PubMed
-
- Fujiwara H, Hoshino T, Yamana K, et al. Number and size of myocytes and amount of interstitial space in the ventricular septum and in the left ventricular free wall in hypertrophic cardiomyopathy. Am J Cardiol 1983;52:818–823. - PubMed
-
- Kaltenbach M, Hopf R, Kunkel B. New Aspects of Hypertrophic Cardiomyopathy: Morphology, Mechanisms and Therapie. Berlin, Germany: Springer Science & Business Media; 2012:421.
-
- Unverferth DV, Baker PB, Pearce LI, et al. Regional myocyte hypertrophy and increased interstitial myocardial fibrosis in hypertrophic cardiomyopathy. Am J Cardiol 1987;59:932–936. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
