

B-cell Therapy for Multiple Sclerosis: Entering an era
- PMID: 29244240
- PMCID: PMC5876115
- DOI: 10.1002/ana.25119
B-cell Therapy for Multiple Sclerosis: Entering an era
Abstract
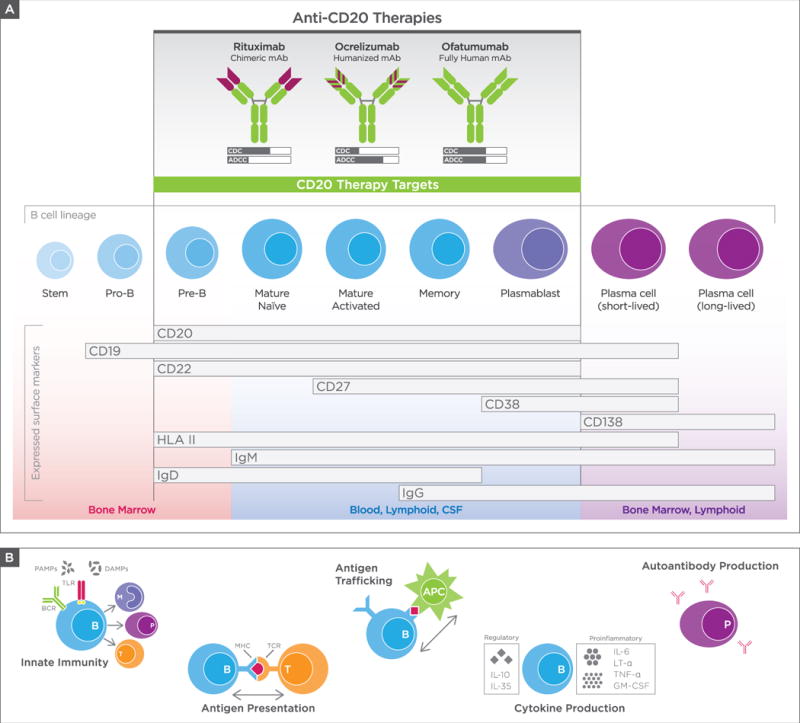
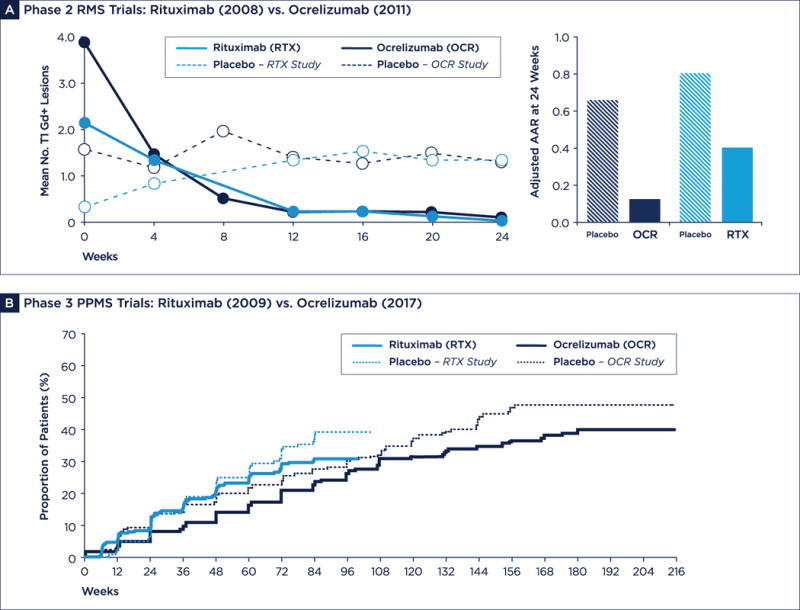
Monoclonal antibodies that target CD20 expressing B cells represent an important new treatment option for patients with multiple sclerosis (MS). B-cell-depleting therapy is highly effective against relapsing forms of the disease and is also the first treatment approach proven to protect against disability worsening in primary progressive MS. Moreover, evolving clinical experience with B-cell therapy, combined with a more sophisticated understanding of humoral immunity in preclinical models and in patients with MS, has led to major progress in deciphering the immune pathogenesis of MS. Here, we review the nuanced roles of B cells in MS autoimmunity, the clinical data supporting use of ocrelizumab and other anti-CD20 therapies in the treatment of MS, as well as safety and practical considerations for prescribing. Last, we summarize remaining unanswered questions regarding the proper role of anti-CD20 therapy in MS, its limitations, and the future landscape of B-cell-based approaches to treatment. Ann Neurol 2018;83:13-26.
© 2017 American Neurological Association.
Conflict of interest statement
No other disclosures were reported.
Figures
References
-
- Hauser SL, Waubant E, Arnold DL, et al. B-cell depletion with rituximab in relapsing-remitting multiple sclerosis. The New England journal of medicine. 2008 Feb 14;358(7):676–88. - PubMed
-
- Montalban X, Hauser SL, Kappos L, et al. Ocrelizumab versus Placebo in Primary Progressive Multiple Sclerosis. The New England journal of medicine. 2017 Jan 19;376(3):209–20. - PubMed
-
- Hauser SL, Bar-Or A, Comi G, et al. Ocrelizumab versus Interferon Beta-1a in Relapsing Multiple Sclerosis. The New England journal of medicine. 2017 Jan 19;376(3):221–34. - PubMed
-
- Dalakas MC. B cells as therapeutic targets in autoimmune neurological disorders. Nature clinical practice Neurology. 2008 Oct;4(10):557–67. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
