

Intervention to improve the appropriate use of polypharmacy for older patients with hip fractures: an observational study
- PMID: 29246247
- PMCID: PMC5732518
- DOI: 10.1186/s12877-017-0681-3
Intervention to improve the appropriate use of polypharmacy for older patients with hip fractures: an observational study
Abstract
Background: Polypharmacy is frequently observed in hip fracture patients. Although it is associated with an increased risk of hip fracture, polypharmacy often continues after hip fracture recovery. This study aimed to evaluate the effectiveness of an intervention to improve appropriate polypharmacy for elderly patients admitted to the hospital for hip fractures.
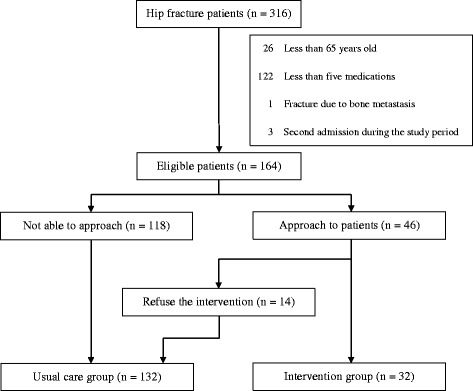
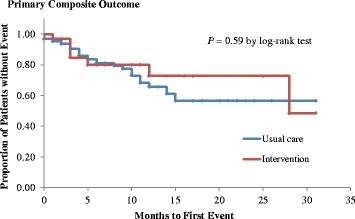
Methods: We conducted a retrospective observational study to compare the outcomes of patients receiving the intervention (n = 32) with those of patients who received usual care (n = 132). All hip fracture patients aged 65 years or older and prescribed 5 or more medications at admission from January 2015 to December 2016 were included in the study. The intervention consisted of an assessment by internal medicine physicians of the appropriateness of polypharmacy and the de-prescription of any unnecessary medications during the patients' hospital stay. The primary composite outcome was death or the first occurrence of any new fracture. Comparisons between the intervention and usual care groups were analyzed using binary logistic regression.
Results: A total of 164 patients were included in the study. The mean patient age was 84.8 years, and the mean numbers of prescribed medications and potentially inappropriate medications at admission were 8.0 and 1.3, respectively. The mean follow-up period was 8.0 months. The primary composite outcome occurred in 35 (21.3%) patients. The total number of potentially inappropriate medications at discharge was significantly lower in the intervention group than in the usual care group (0.8 ± 0.8 for the intervention group vs 1.1 ± 1.0 for the usual care group; p = 0.03). However, no significant differences in the primary composite outcome were found between the intervention and usual care groups (7 in the intervention group and 28 in the usual care group, odds ratio 1.04, 95% CI 0.41-2.65; p = 1.00).
Conclusions: The intervention to improve appropriate polypharmacy was associated with a reduction in potentially inappropriate medications but not an improvement in clinical outcomes. This intervention, which focused only on polypharmacy, may not effectively improve outcomes for elderly patients with hip fractures.
Trial registration: UMIN-CTR UMIN000025495 . Retrospectively registered 2 January 2017.
Keywords: Comorbidity; De-prescription; Hip fractures; Polypharmacy; Potentially inappropriate medication.
Conflict of interest statement
Ethics approval and consent to participate
This study was approved by the Medical Ethical Committee of the National Hospital Organization Tochigi Medical Center. This study was conducted in accordance with the Ethical Guidelines for Epidemiological Research in Japan. We were not required to obtain individual informed consent because we used de-identified data from medical records and did not contact the patients. However, we did display a poster in the waiting room of the hospital to provide information about the collection and use of data for this study and the protection of personal information.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
Prescription of Controlled Substances: Benefits and Risks.2025 Jul 6. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2025 Jul 6. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 30726003 Free Books & Documents.
-
Pharmacist-led deprescribing to improve medication safety in older patients with hip fractures.BMC Geriatr. 2025 Aug 8;25(1):602. doi: 10.1186/s12877-025-06250-8. BMC Geriatr. 2025. PMID: 40781701 Free PMC article.
-
Falls prevention interventions for community-dwelling older adults: systematic review and meta-analysis of benefits, harms, and patient values and preferences.Syst Rev. 2024 Nov 26;13(1):289. doi: 10.1186/s13643-024-02681-3. Syst Rev. 2024. PMID: 39593159 Free PMC article.
-
Multidisciplinary rehabilitation for older people with hip fractures.Cochrane Database Syst Rev. 2021 Nov 12;11(11):CD007125. doi: 10.1002/14651858.CD007125.pub3. Cochrane Database Syst Rev. 2021. PMID: 34766330 Free PMC article.
-
Surgical interventions for treating intracapsular hip fractures in older adults: a network meta-analysis.Cochrane Database Syst Rev. 2022 Feb 14;2(2):CD013404. doi: 10.1002/14651858.CD013404.pub2. Cochrane Database Syst Rev. 2022. PMID: 35156192 Free PMC article.
Cited by
-
Deprescribing medicines in older people living with multimorbidity and polypharmacy: the TAILOR evidence synthesis.Health Technol Assess. 2022 Jul;26(32):1-148. doi: 10.3310/AAFO2475. Health Technol Assess. 2022. PMID: 35894932 Free PMC article. Review.
-
Polypharmacy Management in the Older Adults: A Scoping Review of Available Interventions.Front Pharmacol. 2021 Nov 26;12:734045. doi: 10.3389/fphar.2021.734045. eCollection 2021. Front Pharmacol. 2021. PMID: 34899294 Free PMC article.
-
Potentially inappropriate medication use and associated factors in residents of long-term care facilities: A nationwide cohort study.Front Pharmacol. 2023 Jan 10;13:1092533. doi: 10.3389/fphar.2022.1092533. eCollection 2022. Front Pharmacol. 2023. PMID: 36703731 Free PMC article.
-
Prevalence of potentially inappropriate medications at admission and discharge among hospitalised elderly patients with acute medical illness at a single centre in Japan: a retrospective cross-sectional study.BMJ Open. 2018 Jul 19;8(7):e021152. doi: 10.1136/bmjopen-2017-021152. BMJ Open. 2018. PMID: 30030316 Free PMC article.
-
Association between number of medications and hip fractures in Japanese elderly using conditional logistic LASSO regression.Sci Rep. 2023 Oct 6;13(1):16831. doi: 10.1038/s41598-023-43876-3. Sci Rep. 2023. PMID: 37803071 Free PMC article.
References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
