

Long-term outcome following concomitant mitral valve surgery and Cox maze procedure for atrial fibrillation
- PMID: 29246544
- PMCID: PMC5933444
- DOI: 10.1016/j.jtcvs.2017.09.147
Long-term outcome following concomitant mitral valve surgery and Cox maze procedure for atrial fibrillation
Abstract
Objective: Atrial fibrillation (AF) is associated with increased early and long-term morbidity/mortality following valve surgery. This study examined long-term influence of concomitant full Cox maze (CM) and mitral valve procedures on freedom from atrial arrhythmia and stroke.
Methods: This sample comprised patients who underwent CM with a mitral valve procedure (N = 473). Data on rhythm, medication status, and clinical events captured according to Heart Rhythm Society guidelines at 6, 9, 12, 18, and 24 months and yearly thereafter up to 7 years.
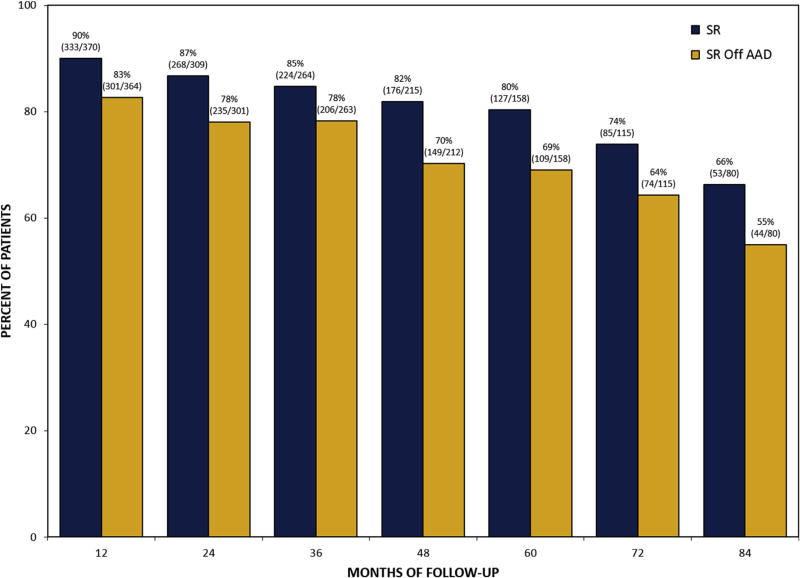
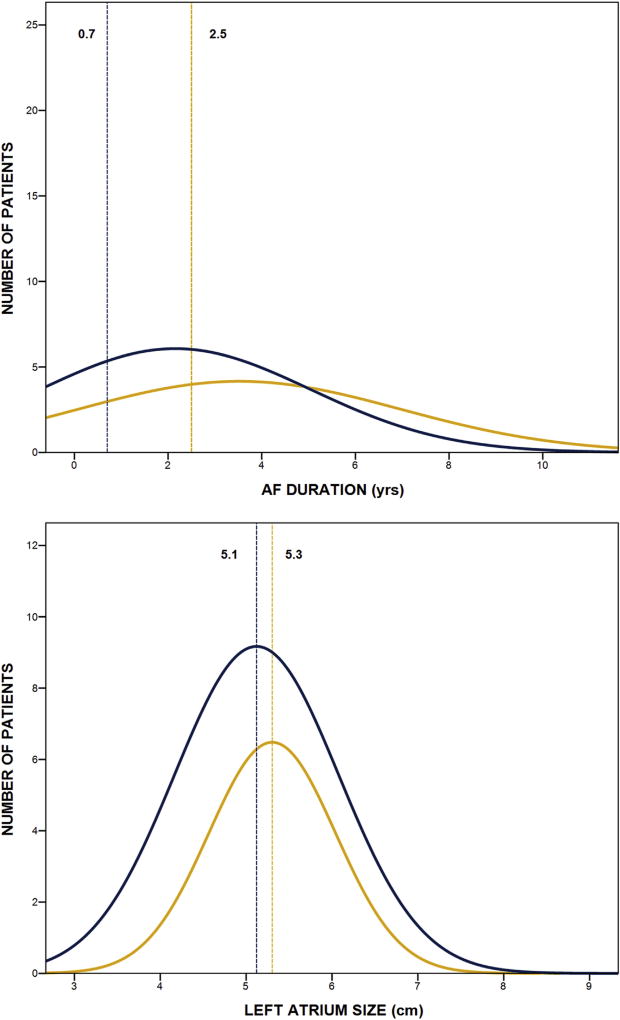
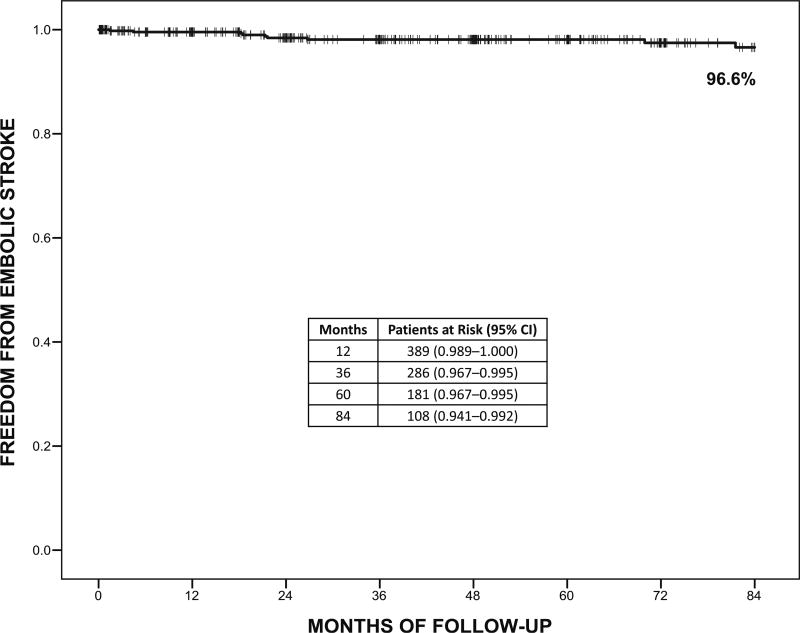
Results: Mean age was 65 years, mean left atrium size was 5.3 cm, and 15% had paroxysmal AF. Perioperative stroke occurred in 2 patients (0.4%) and operative mortality was 2.7% (n = 13). Return to sinus rhythm regardless of antiarrhythmic drugs at 1, 5, and 7 years was 90%, 80%, and 66%. Sinus rhythm off antiarrhythmic drugs at 1, 5, and 7 years was 83%, 69%, and 55%. Freedom from embolic stroke at 7 years was 96.6% (0.4 strokes per 100 patient-years) with a majority of patients off anticoagulation medication. Greater odds of atrial arrhythmia recurrence during 7 years was associated with longer AF duration (odds ratio [OR], 1.07; P = .001), whereas lower odds were associated with cryothermal energy only (OR, 0.64; P = .045) and greater surgeon experience (OR, 0.98; P = .025).
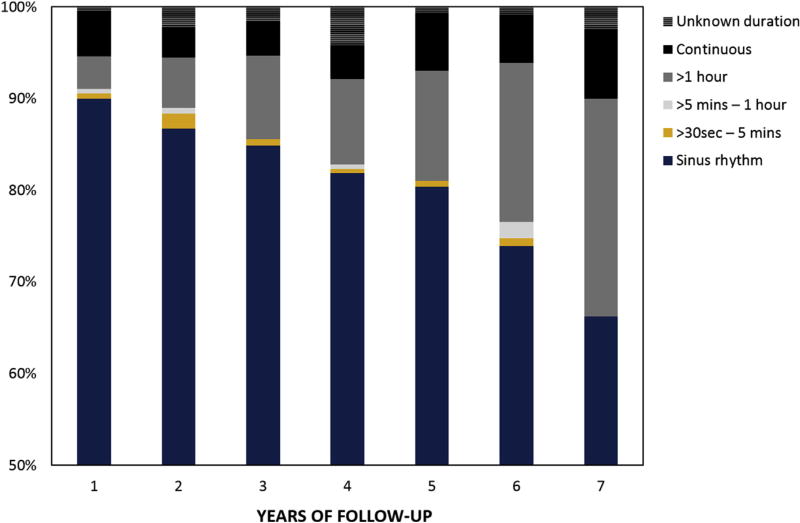
Conclusions: This study suggests that the addition of CM to mitral valve procedures, even with a high degree of complexity, did not increase operative risk. In long-term follow-up, the CM procedure demonstrated acceptable rhythm success, reduced AF burden, and remarkably low stroke rate. Individual surgeon experience and training may notably influence long-term surgical ablation for AF success.
Keywords: atrial fibrillation; cardiac surgery; mitral valve.
Copyright © 2017 The American Association for Thoracic Surgery. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
N.A. is a consultant for Medtronic, a member of the speaker’s bureau for AtriCure, proctor and member of the speaker’s bureau for LivaNova, on the advisory board for Nido Surgical, and co-owner of Left Atrial Appendage Occlusion, LLC. All other authors have nothing to disclose with regard to commercial support.
Figures
Comment in
-
Atrial fibrillation in the patient undergoing mitral valve surgery: A once-in-a-lifetime opportunity.J Thorac Cardiovasc Surg. 2018 Mar;155(3):995-996. doi: 10.1016/j.jtcvs.2017.09.125. Epub 2017 Oct 9. J Thorac Cardiovasc Surg. 2018. PMID: 29089092 No abstract available.
-
Discussion.J Thorac Cardiovasc Surg. 2018 Mar;155(3):992-994. doi: 10.1016/j.jtcvs.2017.09.155. Epub 2017 Dec 13. J Thorac Cardiovasc Surg. 2018. PMID: 29246550 No abstract available.
References
-
- Kannel WB, Abbott RD, Savage DD, McNamara PM. Epidemiologic features of chronic atrial fibrillation: the Framingham study. N Engl J Med. 1982;306:1018–22. - PubMed
-
- Dorian P, Jung W, Newman D, Paquette M, Wood K, Ayers GM, et al. The impairment of health-related quality of life in patients with intermittent atrial fibrillation: implications for the assessment of investigational therapy. J Am Coll Cardiol. 2000;36:1303–9. - PubMed
-
- Chatap G, Giraud K, Vincent JP. Atrial fibrillation in the elderly: Facts and management. Drugs Aging. 2002;19:819–46. - PubMed
-
- Ad N, Suri RM, Gammie JS, Sheng S, O’Brien SM, Henry L. Surgical ablation of atrial fibrillation trends and outcomes in North America. J Thorac Cardiovasc Surg. 2012;144:1051–60. - PubMed
-
- Badhwar V, Rankin JS, Damiano RJ, Gillinov AM, Bakaeen FG, Edgerton JR, et al. The Society of Thoracic Surgeons 2017 clinical practice guidelines for the surgical treatment of atrial fibrillation. Ann Thorac Surg. 2017;103:329–41. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
