

Factors associated with distant recurrence following R0 lobectomy for pN0 lung adenocarcinoma
- PMID: 29246549
- PMCID: PMC5816702
- DOI: 10.1016/j.jtcvs.2017.09.151
Factors associated with distant recurrence following R0 lobectomy for pN0 lung adenocarcinoma
Abstract
Objective: We investigated factors associated with distant recurrence, disease-free survival (DFS), and overall survival (OS) following R0 lobectomy for pathologic node-negative (pN0) lung adenocarcinoma.
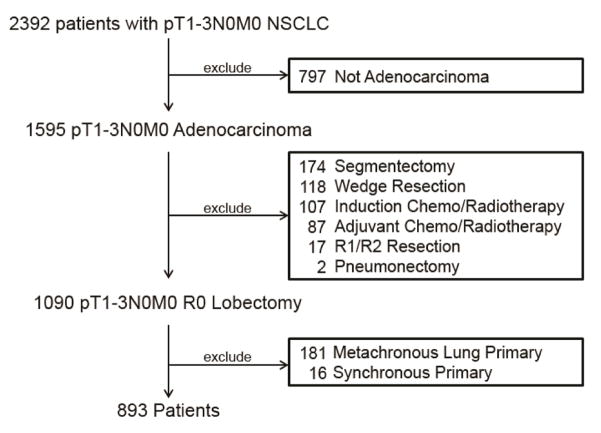
Methods: We performed a retrospective analysis of a prospectively maintained database of patients with pT1-3N0M0 non-small cell lung cancer. Exclusion criteria included metachronous lung cancer, sublobar/incomplete resection, nonadenocarcinoma histology, and induction/adjuvant therapy. The primary outcome was distant recurrence; secondary outcomes were DFS and OS. Associations between variables and outcomes were assessed by Fine-Gray competing-risk regression for distant recurrence and Cox proportional hazard models for DFS and OS.
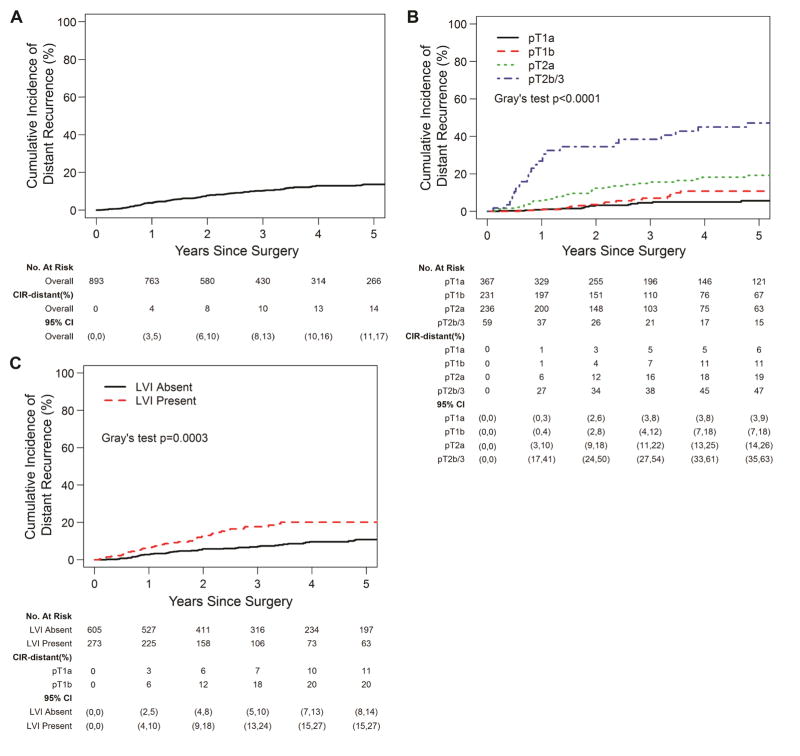
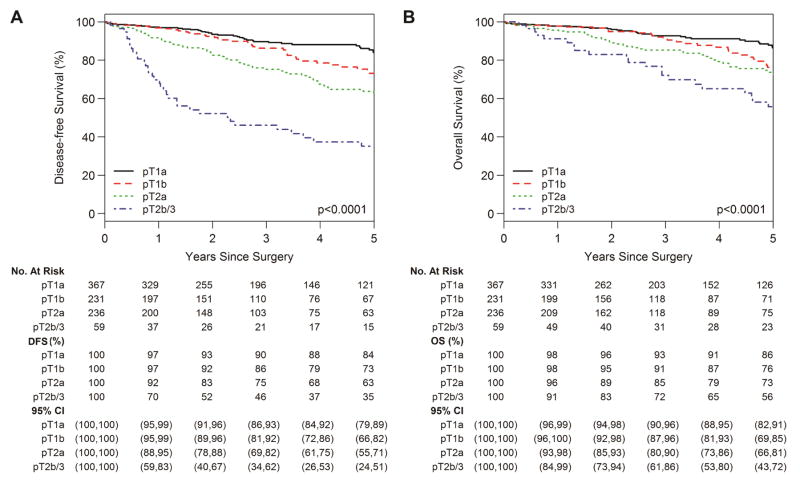
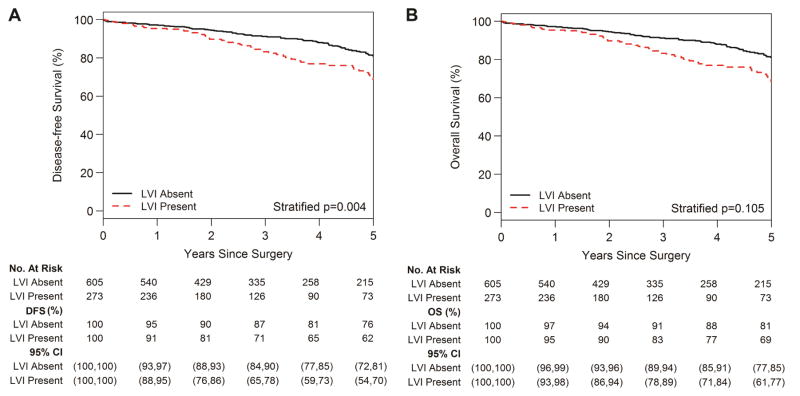
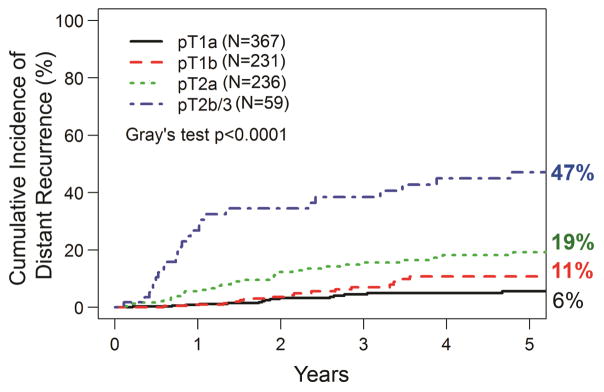
Results: Of 2392 patients identified with pT1-3N0M0 lung adenocarcinoma, 893 met the inclusion criteria. Median follow-up was 35.0 months (range, 0.1-202 months). Thirteen percent of patients developed recurrence (n = 115), of which 86% (n = 99) were distant. The 5-year cumulative incidence of distant recurrence was 14% (95% confidence interval [CI], 11%-17%). On multivariable analysis, pT2a (hazard ratio [HR], 2.84; 95% CI, 1.56-5.16; P = .001) and pT2b/3 (HR, 6.53; 95% CI, 3.17-13.5; P < .001) tumors were associated with distant recurrence. Recent surgery was associated with decreased distant recurrence (HR, 0.43; 95% CI, 0.20-0.91; P = .028), and lymphovascular invasion was strongly associated with distant recurrence (HR, 1.62; 95% CI, 1.00-2.63; P = .05). DFS was independently associated with pT stage (P < .001) and lymphovascular invasion (P = .004).
Conclusions: In patients undergoing R0 lobectomy with pN0 lung adenocarcinoma, pT stage and lymphovascular invasion were associated with distant recurrence and decreased DFS. These observations support the inclusion of these patients in future clinical trials investigating adjuvant targeted and immunotherapies.
Keywords: lobectomy; lung adenocarcinoma; lymphovascular invasion; pathologic tumor stage; recurrence.
Copyright © 2017 The American Association for Thoracic Surgery. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
Comment in
-
Rearranging the deck chairs.J Thorac Cardiovasc Surg. 2018 Mar;155(3):1205. doi: 10.1016/j.jtcvs.2017.10.019. Epub 2017 Oct 20. J Thorac Cardiovasc Surg. 2018. PMID: 29100585 No abstract available.
-
Discussion.J Thorac Cardiovasc Surg. 2018 Mar;155(3):1222-1224. doi: 10.1016/j.jtcvs.2017.09.159. Epub 2017 Dec 13. J Thorac Cardiovasc Surg. 2018. PMID: 29246548 No abstract available.
-
Risk stratification for distant recurrence of resected early stage non-small cell lung cancer is under construction.J Thorac Cardiovasc Surg. 2018 Mar;155(3):1225-1226. doi: 10.1016/j.jtcvs.2017.10.063. Epub 2017 Nov 1. J Thorac Cardiovasc Surg. 2018. PMID: 29305028 No abstract available.
-
Visiting an old foe: distant recurrence following R0 lobectomy for pathological N0 lung adenocarcinoma.J Thorac Dis. 2018 Sep;10(Suppl 26):S3286-S3289. doi: 10.21037/jtd.2018.08.116. J Thorac Dis. 2018. PMID: 30370139 Free PMC article. No abstract available.
References
-
- Goldstraw P, Chansky K, Crowley J, Rami-Porta R, Asamura H, Eberhardt WE, et al. The IASLC Lung Cancer Staging Project: Proposals for Revision of the TNM Stage Groupings in the Forthcoming (Eighth) Edition of the TNM Classification for Lung Cancer. J Thorac Oncol. 2016;11:39–51. - PubMed
-
- Hancock JG, Rosen JE, Antonicelli A, Moreno A, Kim AW, Detterbeck FC, et al. Impact of adjuvant treatment for microscopic residual disease after non-small cell lung cancer surgery. Ann Thorac Surg. 2015;99:406–413. - PubMed
-
- Ginsberg RJ, Rubinstein LV. Randomized trial of lobectomy versus limited resection for T1 N0 non-small cell lung cancer. Lung Cancer Study Group. Ann Thorac Surg. 1995;60:615–622. discussion 622–613. - PubMed
-
- Dai C, Shen J, Ren Y, Zhong S, Zheng H, He J, et al. Choice of Surgical Procedure for Patients With Non-Small-Cell Lung Cancer </= 1 cm or > 1 to 2 cm Among Lobectomy, Segmentectomy, and Wedge Resection: A Population-Based Study. J Clin Oncol. 2016;34:3175–3182. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
