

The Management of Myelomeningocele Study: full cohort 30-month pediatric outcomes
- PMID: 29246577
- PMCID: PMC7737375
- DOI: 10.1016/j.ajog.2017.12.001
The Management of Myelomeningocele Study: full cohort 30-month pediatric outcomes
Abstract
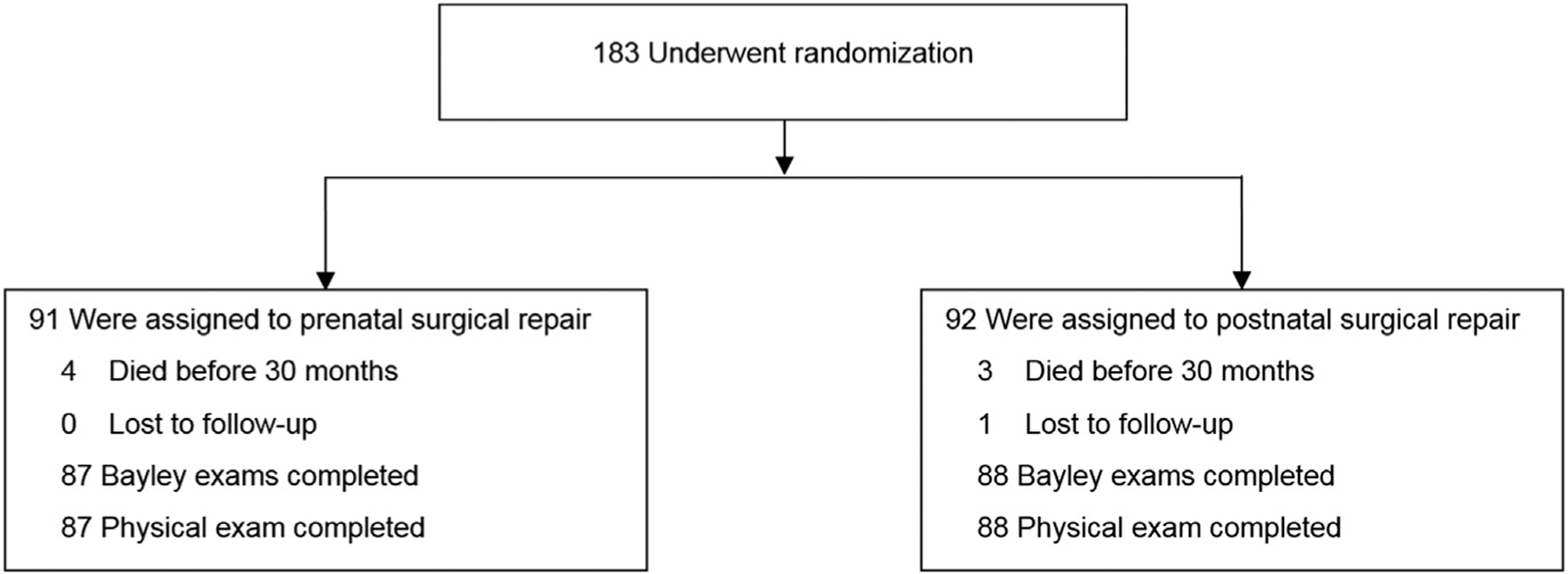
Background: Previous reports from the Management of Myelomeningocele Study demonstrated that prenatal repair of myelomeningocele reduces hindbrain herniation and the need for cerebrospinal fluid shunting, and improves motor function in children with myelomeningocele. The trial was stopped for efficacy after 183 patients were randomized, but 30-month outcomes were only available at the time of initial publication in 134 mother-child dyads. Data from the complete cohort for the 30-month outcomes are presented here. Maternal and 12-month neurodevelopmental outcomes for the full cohort were reported previously.
Objective: The purpose of this study is to report the 30-month outcomes for the full cohort of patients randomized to either prenatal or postnatal repair of myelomeningocele in the original Management of Myelomeningocele Study.
Study design: Eligible women were randomly assigned to undergo standard postnatal repair or prenatal repair <26 weeks gestation. We evaluated a composite of mental development and motor function outcome at 30 months for all enrolled patients as well as independent ambulation and the Bayley Scales of Infant Development, Second Edition. We assessed whether there was a differential effect of prenatal surgery in subgroups defined by: fetal leg movements, ventricle size, presence of hindbrain herniation, gender, and location of the myelomeningocele lesion. Within the prenatal surgery group only, we evaluated these and other baseline parameters as predictors of 30-month motor and cognitive outcomes. We evaluated whether presence or absence of a shunt at 1 year was associated with 30-month motor outcomes.
Results: The data for the full cohort of 183 patients corroborate the original findings of Management of Myelomeningocele Study, confirming that prenatal repair improves the primary outcome composite score of mental development and motor function (199.4 ± 80.5 vs 166.7 ± 76.7, P = .004). Prenatal surgery also resulted in improvement in the secondary outcomes of independent ambulation (44.8% vs 23.9%, P = .004), WeeFIM self-care score (20.8 vs 19.0, P = .006), functional level at least 2 better than anatomic level (26.4% vs 11.4%, P = .02), and mean Bayley Scales of Infant Development, Second Edition, psychomotor development index (17.3% vs 15.1%, P = .03), but does not affect cognitive development at 30 months. On subgroup analysis, there was a nominally significant interaction between gender and surgery, with boys demonstrating better improvement in functional level and psychomotor development index. For patients receiving prenatal surgery, the presence of in utero ankle, knee, and hip movement, absence of a sac over the lesion and a myelomeningocele lesion of ≤L3 were significantly associated with independent ambulation. Postnatal motor function showed no correlation with either prenatal ventricular size or postnatal shunt placement.
Conclusion: The full cohort data of 30-month cognitive development and motor function outcomes validate in utero surgical repair as an effective treatment for fetuses with myelomeningocele. Current data suggest that outcomes related to the need for shunting should be counseled separately from the outcomes related to distal neurologic functioning.
Keywords: Management of Myelomeningocele Study; and hip movement; ankle; fetal surgery; knee; long-term follow-up; motor outcomes; myelomeningocele; postnatal motor function; shunt; ventricular size; ventriculomegaly.
Copyright © 2017 Elsevier Inc. All rights reserved.
Conflict of interest statement
The authors report no conflict of interest.
Figures
Comment in
-
Prenatal superior to postnatal myelomeningocele surgery.J Pediatr. 2018 Jul;198:322-325. doi: 10.1016/j.jpeds.2018.04.060. J Pediatr. 2018. PMID: 29936963 No abstract available.
-
A clinician's concerns about motor function outcomes of fetal surgery for myelomeningocele.Am J Obstet Gynecol. 2019 Jan;220(1):124. doi: 10.1016/j.ajog.2018.09.020. Epub 2018 Sep 19. Am J Obstet Gynecol. 2019. PMID: 30243606 No abstract available.
-
Reply.Am J Obstet Gynecol. 2019 Jan;220(1):125. doi: 10.1016/j.ajog.2018.09.022. Epub 2018 Sep 21. Am J Obstet Gynecol. 2019. PMID: 30248309 No abstract available.
References
-
- Ouyang L, Grosse SD, Armour BS, Waitzman NJ. Health care expenditures of children and adults with spina bifida in a privately insured US population. Birth Defects Res A Clin Mol Teratol 2007;79:552–8. - PubMed
-
- Centers for Disease Control. Economic burden of spina bifida–United States, 19801990. MMWR Morb Mortal Wkly Rep 1989;38: 264–7. - PubMed
-
- Farmer DL, von Koch CS, Peacock WJ, et al. In-utero repair of myelomeningocele: experimental pathophysiology, initial clinical experience, and outcomes. Arch Surg 2003;138: 872–8. - PubMed
-
- Johnson MP, Sutton LN, Rintoul N, et al. Fetal myelomeningocele repair: short-term clinical outcomes. Am J Obstet Gynecol 2003;189: 482–7. - PubMed
-
- Johnson MP, Gerdes M, Rintoul N, et al. Maternal-fetal surgery for myelomeningocele: neurodevelopmental outcomes at 2 years of age. Am J Obstet Gynecol 2006;194:1145–52. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
