

Associations of Lipoprotein(a) Levels With Incident Atrial Fibrillation and Ischemic Stroke: The ARIC (Atherosclerosis Risk in Communities) Study
- PMID: 29246963
- PMCID: PMC5779047
- DOI: 10.1161/JAHA.117.007372
Associations of Lipoprotein(a) Levels With Incident Atrial Fibrillation and Ischemic Stroke: The ARIC (Atherosclerosis Risk in Communities) Study
Abstract
Background: Lipoprotein(a) (Lp[a]) is proatherosclerotic and prothrombotic, causally related to coronary disease, and associated with other cardiovascular diseases. The association of Lp(a) with incident atrial fibrillation (AF) and with ischemic stroke among individuals with AF remains to be elucidated.
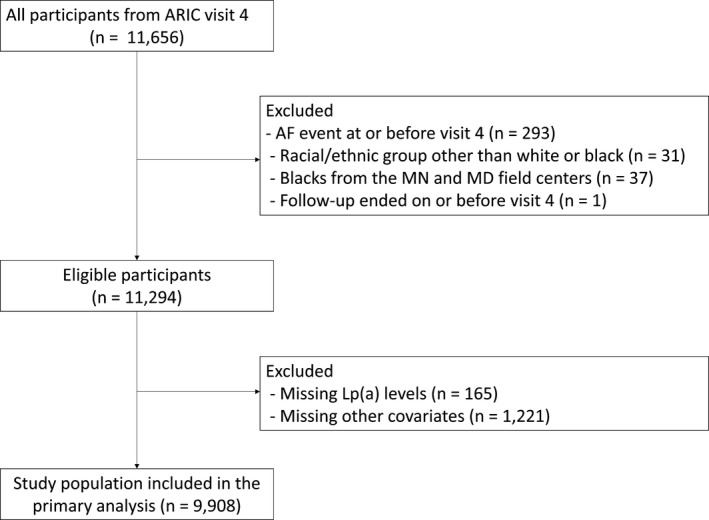
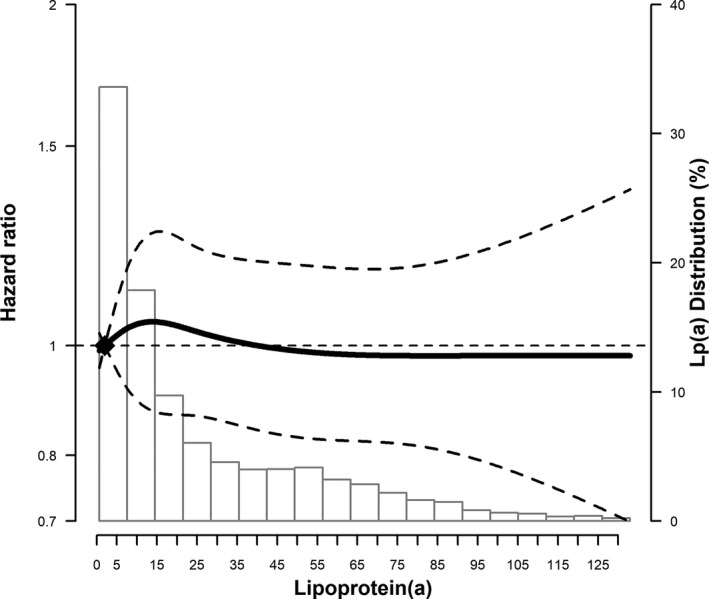
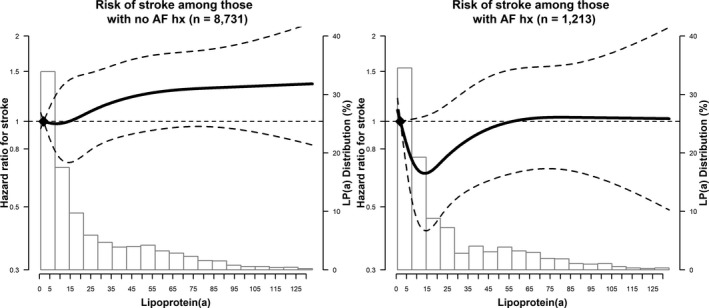
Methods and results: In the community-based ARIC (Atherosclerosis Risk in Communities) study cohort, Lp(a) levels were measured by a Denka Seiken assay at visit 4 (1996-1998). We used multivariable-adjusted Cox models to compare AF and ischemic stroke risk across Lp(a) levels. First, we evaluated incident AF in 9908 participants free of AF at baseline. AF was ascertained by electrocardiography at study visits, hospital International Statistical Classification of Diseases, 9th Revision (ICD-9) codes, and death certificates. We then evaluated incident ischemic stroke in 10 127 participants free of stroke at baseline. Stroke was identified by annual phone calls, hospital ICD-9 Revision codes, and death certificates. The baseline age was 62.7±5.6 years. Median Lp(a) levels were 13.3 mg/dL (interquartile range, 5.2-39.7 mg/dL). Median follow-up was 13.9 and 15.8 years for AF and stroke, respectively. Lp(a) was not associated with incident AF (hazard ratio, 0.98; 95% confidence interval, 0.82-1.17), comparing those with Lp(a) ≥50 with those with Lp(a) <10 mg/dL. High Lp(a) was associated with a 42% relative increase in stroke risk among participants without AF (hazard ratio, 1.42; 95% confidence interval, 1.07-1.90) but not in those with AF (hazard ratio, 1.06; 95% confidence interval, 0.70-1.61 [P interaction for AF=0.25]). There were no interactions by race or sex. No association was found for cardioembolic stroke subtype.
Conclusions: High Lp(a) levels were not associated with incident AF. Lp(a) levels were associated with increased ischemic stroke risk, primarily among individuals without AF but not in those with AF.
Keywords: atrial fibrillation; cardioembolic stroke; epidemiology; lipoprotein; lipoprotein (a); risk factor; stroke.
© 2017 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley.
Figures

References
-
- Fless GM, Rolih CA, Scanu AM. Heterogeneity of human plasma lipoprotein (a). Isolation and characterization of the lipoprotein subspecies and their apoproteins. J Biol Chem. 1984;259:11470–11478. - PubMed
-
- McLean JW, Tomlinson JE, Kuang WJ, Eaton DL, Chen EY, Fless GM, Scanu AM, Lawn RM. cDNA sequence of human apolipoprotein(a) is homologous to plasminogen. Nature. 1987;330:132–137. - PubMed
-
- Caplice NM, Panetta C, Peterson TE, Kleppe LS, Mueske CS, Kostner GM, Broze GJ Jr, Simari RD. Lipoprotein (a) binds and inactivates tissue factor pathway inhibitor: a novel link between lipoproteins and thrombosis. Blood. 2001;98:2980–2987. - PubMed
-
- Danesh J, Collins R, Peto R. Lipoprotein(a) and coronary heart disease. Meta‐analysis of prospective studies. Circulation. 2000;102:1082–1085. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
