

The immunology of hypertension
- PMID: 29247045
- PMCID: PMC5748862
- DOI: 10.1084/jem.20171773
The immunology of hypertension
Erratum in
-
Correction: The immunology of hypertension.J Exp Med. 2018 Feb 5;215(2):719. doi: 10.1084/jem.2017177301022018c. Epub 2018 Jan 5. J Exp Med. 2018. PMID: 29305396 Free PMC article. No abstract available.
Abstract
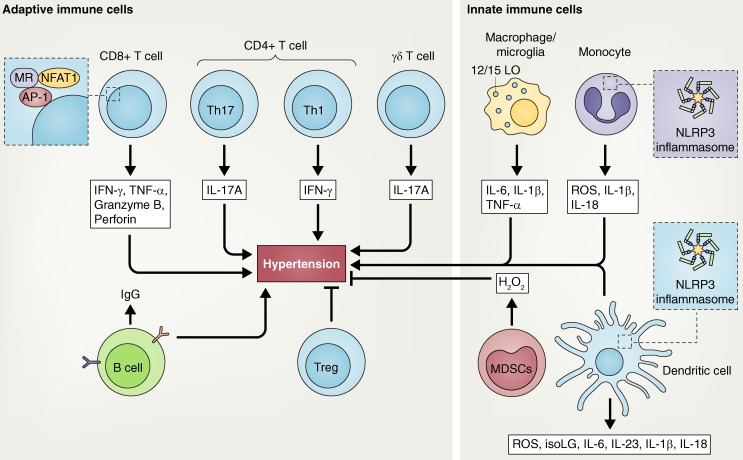
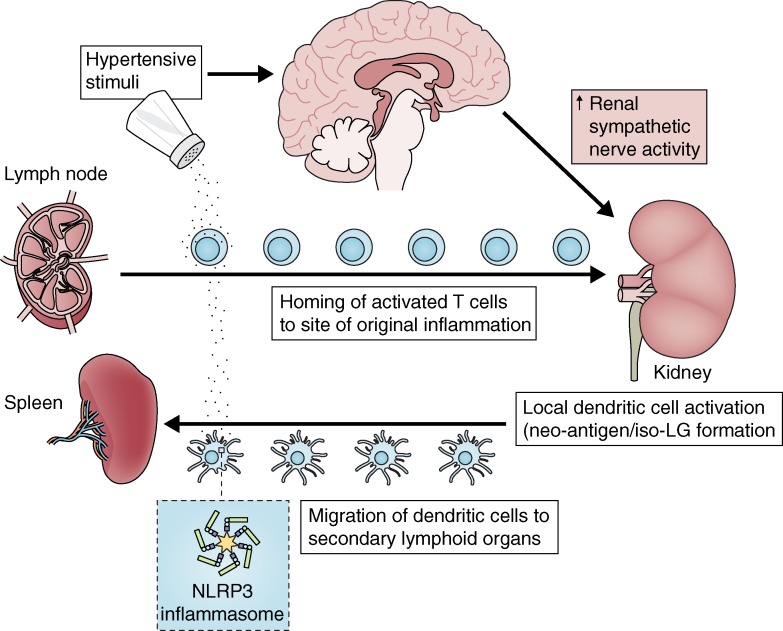
Although systemic hypertension affects a large proportion of the population, its etiology remains poorly defined. Emerging evidence supports the concept that immune cells become activated and enter target organs, including the vasculature and the kidney, in this disease. Mediators released by these cells, including reactive oxygen species, metalloproteinases, cytokines, and antibodies promote dysfunction of the target organs and cause damage. In vessels, these factors enhance constriction, remodeling, and rarefaction. In the kidney, these mediators increase expression and activation of sodium transporters, and cause interstitial fibrosis and glomerular injury. Factors common to hypertension, including oxidative stress, increased interstitial sodium, cytokine production, and inflammasome activation promote immune activation in hypertension. Recent data suggest that isolevuglandin-modified self-proteins in antigen-presenting cells are immunogenic, promoting cytokine production by the cells in which they are formed and T cell activation. Efforts to prevent and reverse immune activation may prove beneficial in preventing the long-term sequelae of hypertension and its related cardiovascular diseases.
© 2018 Norlander et al.
Figures

References
-
- Amador C.A., Barrientos V., Peña J., Herrada A.A., González M., Valdés S., Carrasco L., Alzamora R., Figueroa F., Kalergis A.M., and Michea L.. 2014. Spironolactone decreases DOCA-salt-induced organ damage by blocking the activation of T helper 17 and the downregulation of regulatory T lymphocytes. Hypertension. 63:797–803. 10.1161/HYPERTENSIONAHA.113.02883 - DOI - PubMed
-
- Ba D., Takeichi N., Kodama T., and Kobayashi H.. 1982. Restoration of T cell depression and suppression of blood pressure in spontaneously hypertensive rats (SHR) by thymus grafts or thymus extracts. J. Immunol. 128:1211–1216. - PubMed
-
- Barbaro N.R., Foss J.D., Kryshtal D.O., Tsyba N., Kumaresan S., Xiao L., Mernaugh R.L., Itani H.A., Loperena R., Chen W., et al. 2017. Dendritic cell amiloride-sensitive channels mediate sodium-induced inflammation and hypertension. Cell Reports. 21:1009–1020. 10.1016/j.celrep.2017.10.002 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
