

Novel Telestroke Program Improves Thrombolysis for Acute Stroke Across 21 Hospitals of an Integrated Healthcare System
- PMID: 29247142
- PMCID: PMC5753819
- DOI: 10.1161/STROKEAHA.117.018413
Novel Telestroke Program Improves Thrombolysis for Acute Stroke Across 21 Hospitals of an Integrated Healthcare System
Abstract
Background and purpose: Faster treatment with intravenous alteplase in acute ischemic stroke is associated with better outcomes. Starting in 2015, Kaiser Permanente Northern California redesigned its acute stroke workflow across all 21 Kaiser Permanente Northern California stroke centers to (1) follow a single standardized version of a modified Helsinki model and (2) have all emergency stroke cases managed by a dedicated telestroke neurologist. We examined the effect of Kaiser Permanente Northern California's Stroke EXpediting the PRrocess of Evaluating and Stopping Stroke program on door-to-needle (DTN) time, alteplase use, and symptomatic intracranial hemorrhage rates.
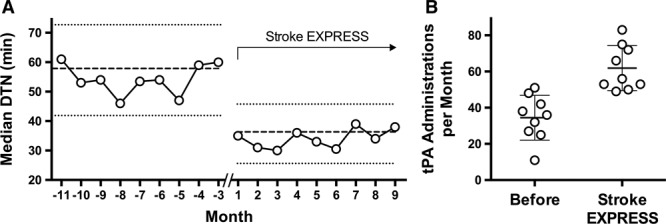
Methods: The program was introduced in a staggered fashion from September 2015 to January 2016. We compared DTN times for a seasonally adjusted 9-month period at each center before implementation to the corresponding 9-month calendar period from the start of implementation. The primary outcome was the DTN time for alteplase administration. Secondary outcomes included rate of alteplase administrations per month, symptomatic intracranial hemorrhage, and disposition at time of discharge.
Results: This study included 310 patients treated with alteplase in the pre-EXpediting the PRrocess of Evaluating and Stopping Stroke period and 557 patients treated with alteplase in the EXpediting the PRrocess of Evaluating and Stopping Stroke period. After implementation, alteplase administrations increased to 62/mo from 34/mo at baseline (P<0.001). Median DTN time decreased to 34 minutes after implementation from 53.5 minutes prior (P<0.001), and DTN time of <60 minutes was achieved in 87.1% versus 61.0% (P<0.001) of patients. DTN times <30 minutes were much more common in the Stroke EXpediting the PRrocess of Evaluating and Stopping Stroke period (40.8% versus 4.2% before implementation). There was no significant difference in symptomatic intracranial hemorrhage rates in the 2 periods (3.8% versus 2.2% before implementation; P=0.29).
Conclusions: Introduction of a standardized modified Helsinki protocol across 21 hospitals using telestroke management was associated with increased alteplase administrations, significantly shorter DTN times, and no increase in adverse outcomes.
Keywords: acute stroke care; intracranial hemorrhages; stroke; telemedicine; time-to-treatment; tissue-type plasminogen activator.
© 2017 The Authors.
Figures
References
-
- Saver JL. Time is brain–quantified. Stroke. 2006;37:263–266. doi: 10.1161/01.STR.0000196957.55928.ab. - PubMed
-
- Meretoja A, Keshtkaran M, Saver JL, Tatlisumak T, Parsons MW, Kaste M, et al. Stroke thrombolysis: save a minute, save a day. Stroke. 2014;45:1053–1058. doi: 10.1161/STROKEAHA.113.002910. - PubMed
-
- Fonarow GC, Smith EE, Saver JL, Reeves MJ, Hernandez AF, Peterson ED, et al. Improving door-to-needle times in acute ischemic stroke. Stroke. 2011;42:2983–2989. - PubMed
-
- Meretoja A, Strbian D, Mustanoja S, Tatlisumak T, Lindsberg PJ, Kaste M. Reducing in-hospital delay to 20 minutes in stroke thrombolysis. Neurology. 2012;79:306–313. doi: 10.1212/WNL.0b013e31825d6011. - PubMed
-
- Meretoja A, Weir L, Ugalde M, Yassi N, Yan B, Hand P, et al. Helsinki model cut stroke thrombolysis delays to 25 minutes in Melbourne in only 4 months. Neurology. 2013;81:1071–1076. doi: 10.1212/WNL.0b013e3182a4a4d2. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
