

Computer-Aided Nodule Assessment and Risk Yield (CANARY) may facilitate non-invasive prediction of EGFR mutation status in lung adenocarcinomas
- PMID: 29247171
- PMCID: PMC5732170
- DOI: 10.1038/s41598-017-17659-6
Computer-Aided Nodule Assessment and Risk Yield (CANARY) may facilitate non-invasive prediction of EGFR mutation status in lung adenocarcinomas
Abstract
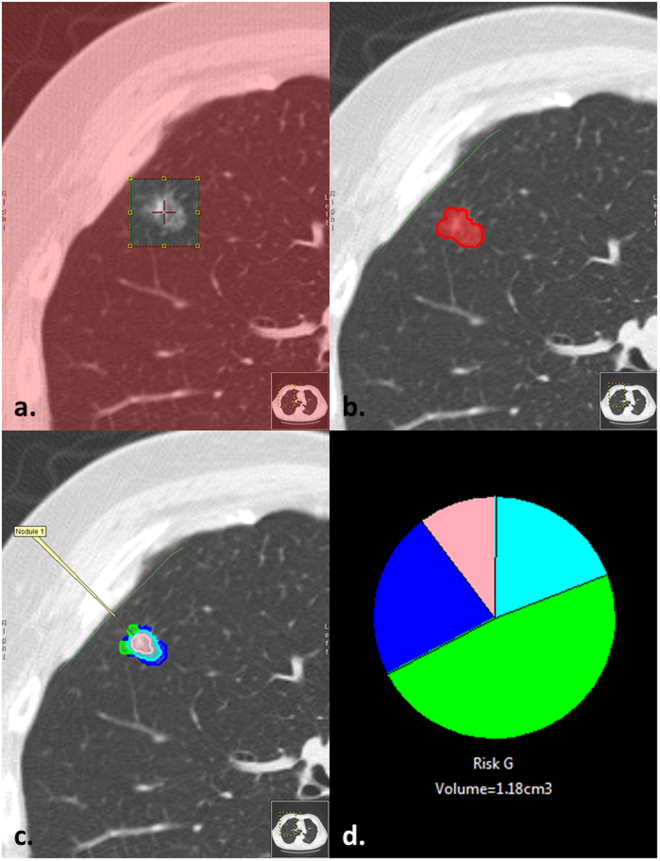
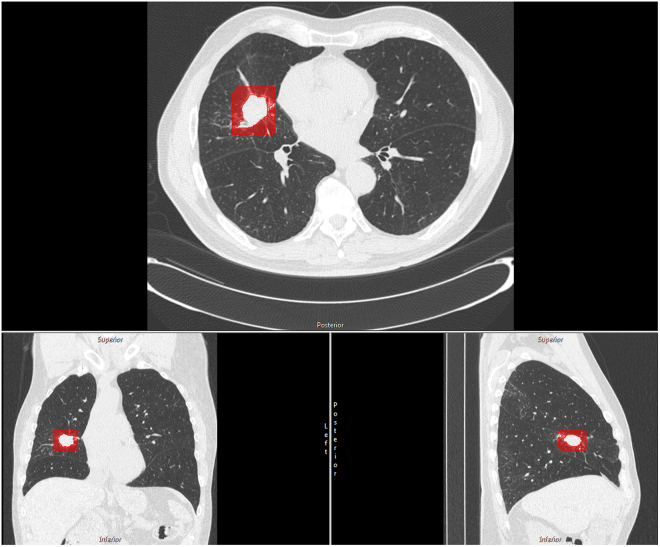
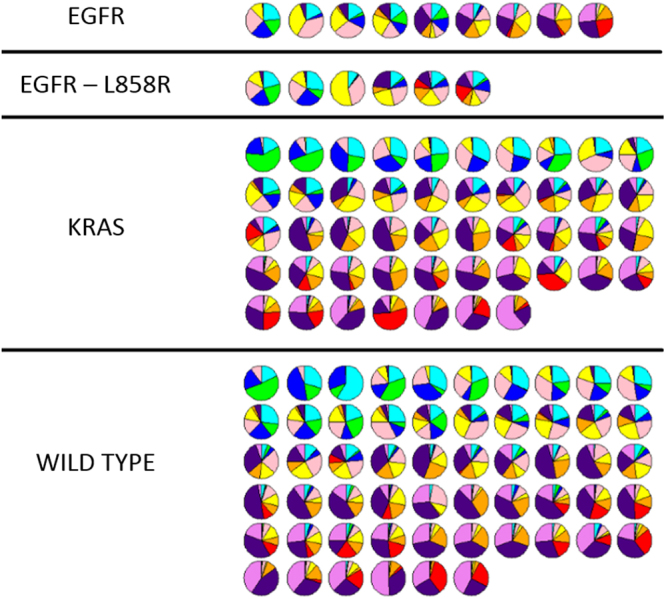
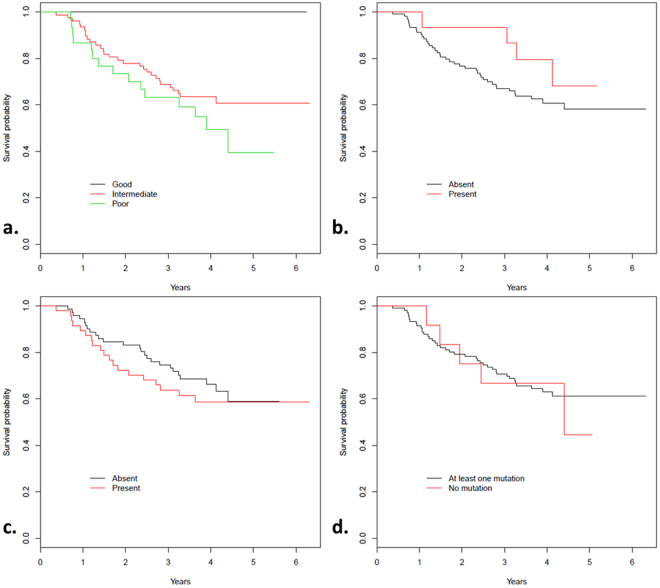
Computer-Aided Nodule Assessment and Risk Yield (CANARY) is quantitative imaging analysis software that predicts the histopathological classification and post-treatment disease-free survival of patients with adenocarcinoma of the lung. CANARY characterizes nodules by the distribution of nine color-coded texture-based exemplars. We hypothesize that quantitative computed tomography (CT) analysis of the tumor and tumor-free surrounding lung facilitates non-invasive identification of clinically-relevant mutations in lung adenocarcinoma. Comprehensive analysis of targetable mutations (50-gene-panel) and CANARY analysis of the preoperative (≤3 months) high resolution CT (HRCT) was performed for 118 pulmonary nodules of the adenocarcinoma spectrum surgically resected between 2006-2010. Logistic regression with stepwise variable selection was used to determine predictors of mutations. We identified 140 mutations in 106 of 118 nodules. TP53 (n = 48), KRAS (n = 47) and EGFR (n = 15) were the most prevalent. The combination of Y (Yellow) and G (Green) exemplars, fibrosis within the surrounding lung and smoking status were the best discriminators for an EGFR mutation (AUC 0.77 and 0.87, respectively). None of the EGFR mutants expressing TP53 (n = 5) had a good prognosis based on CANARY features. No quantitative features were significantly associated with KRAS mutations. Our exploratory analysis indicates that quantitative CT analysis of a nodule and surrounding lung may noninvasively predict the presence of EGFR mutations in pulmonary nodules of the adenocarcinoma spectrum.
Conflict of interest statement
CANARY software, currently licensed to Imbio LLC (annual royalties <$5000). This COI applies to Mayo Clinic and Brian Bartholmai, Fabien Maldonado, Ron Karwoski, Tobias Peikert and Srinivasan Rajagopalan. Ryan Clay, Benjamin Kipp, Jesse Voss and Marie Christine Aubry have no relevant conflicts of interest to disclose.
Figures
References
-
- Moyer VA, Force USPST. Screening for lung cancer: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med. 2014;160:330–338. - PubMed
-
- Zhou C, et al. Erlotinib versus chemotherapy as first-line treatment for patients with advanced EGFR mutation-positive non-small-cell lung cancer (OPTIMAL, CTONG-0802): a multicentre, open-label, randomised, phase 3 study. Lancet Oncol. 2011;12:735–742. doi: 10.1016/S1470-2045(11)70184-X. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
