

Anti-Mullerian Hormone-to-Testosterone Ratio is Predictive of Positive Sperm Retrieval in Men with Idiopathic Non-Obstructive Azoospermia
- PMID: 29247212
- PMCID: PMC5732204
- DOI: 10.1038/s41598-017-17420-z
Anti-Mullerian Hormone-to-Testosterone Ratio is Predictive of Positive Sperm Retrieval in Men with Idiopathic Non-Obstructive Azoospermia
Abstract
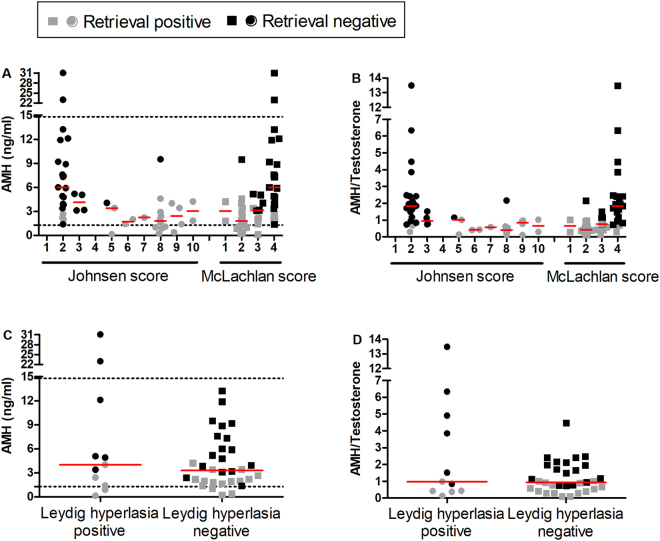
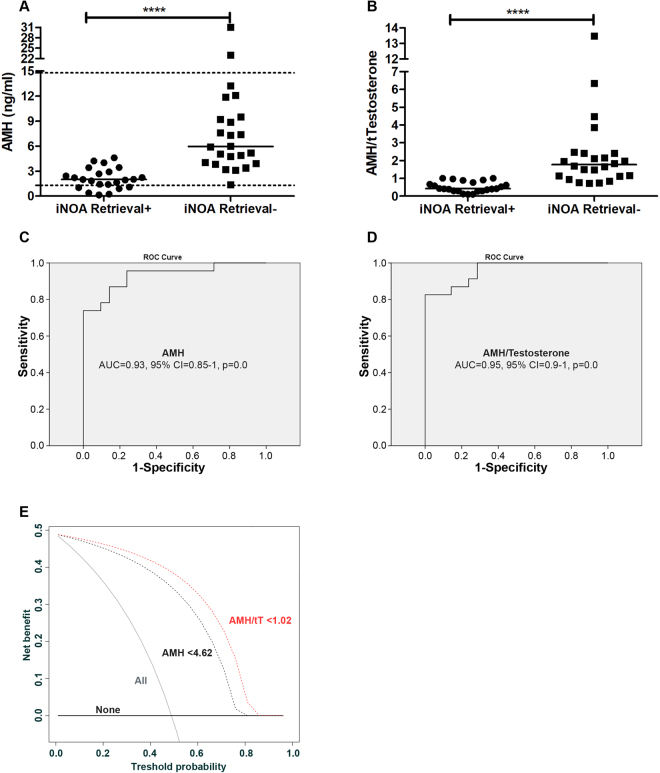
The lack of clinically-reliable biomarkers makes impossible to predict sperm retrieval outcomes at testicular sperm extraction (TESE) in men with non-obstructive azoospermia (NOA), resulting in up to 50% of unnecessary surgical interventions. Clinical data, hormonal profile and histological classification of testis parenchyma from 47 white-Caucasian idiopathic NOA (iNOA) men submitted to microdissection TESE (microTESE) were analyzed. Logistic regression analyses tested potential clinical predictors of positive sperm retrieval. The predictive accuracy of all variables was evaluated using the receiver operating characteristic-derived area under the curve, and the clinical net benefit estimated by a decision-curve analysis (DCA). Overall, 23 (49%) and 24 (51%) patients were classified as positive and negative sperm retrievals at microTESE. While circulating hormones associated to a condition of primary hypogonadism did not predict sperm retrieval, levels of anti-Mullerian hormone (AMH) and the ratio AMH-to-total Testosterone (AMH/tT) achieved independent predictor status for sperm retrieval at microTESE, with a predictive accuracy of 93% and 95%. Using cutoff values of <4.62 ng/ml for AMH and <1.02 for AMH/tT, positive sperm retrieval was predicted in all individuals, with 19 men out of 47 potentially spared from surgery. DCA findings demonstrated clinical net benefit using AMH and AMH/tT for patient selection at microTESE.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Jungwirth A. et al. Guidelines on male infertility. European Urology Association. http://uroweb.org/guideline/male-infertility/ (2015).
-
- World Health Organization, Department of Reproductive Health and Research. WHO Laboratory Manual for the Examination and Processing of Human Semen. Fifth edition. who.int/publications/2010/9789241547789_eng.pdf (2010).
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
