

Estimates of global seasonal influenza-associated respiratory mortality: a modelling study
- PMID: 29248255
- PMCID: PMC5935243
- DOI: 10.1016/S0140-6736(17)33293-2
Estimates of global seasonal influenza-associated respiratory mortality: a modelling study
Erratum in
-
Department of Error.Lancet. 2018 Mar 31;391(10127):1262. doi: 10.1016/S0140-6736(18)30105-3. Epub 2018 Jan 19. Lancet. 2018. PMID: 29370997 No abstract available.
Abstract
Background: Estimates of influenza-associated mortality are important for national and international decision making on public health priorities. Previous estimates of 250 000-500 000 annual influenza deaths are outdated. We updated the estimated number of global annual influenza-associated respiratory deaths using country-specific influenza-associated excess respiratory mortality estimates from 1999-2015.
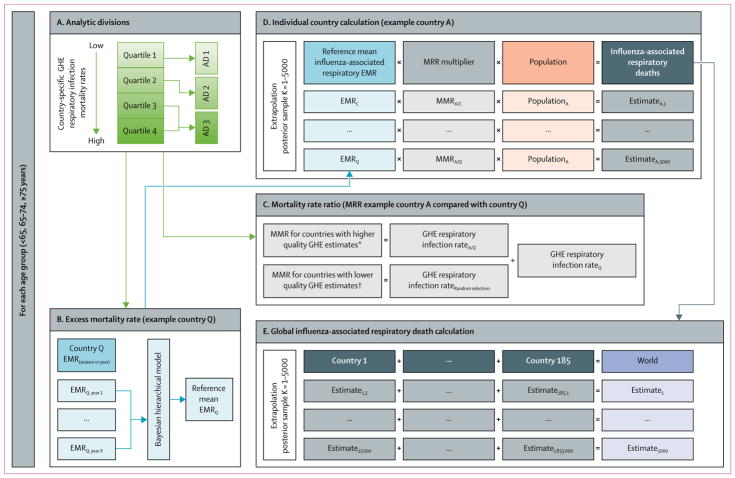
Methods: We estimated country-specific influenza-associated respiratory excess mortality rates (EMR) for 33 countries using time series log-linear regression models with vital death records and influenza surveillance data. To extrapolate estimates to countries without data, we divided countries into three analytic divisions for three age groups (<65 years, 65-74 years, and ≥75 years) using WHO Global Health Estimate (GHE) respiratory infection mortality rates. We calculated mortality rate ratios (MRR) to account for differences in risk of influenza death across countries by comparing GHE respiratory infection mortality rates from countries without EMR estimates with those with estimates. To calculate death estimates for individual countries within each age-specific analytic division, we multiplied randomly selected mean annual EMRs by the country's MRR and population. Global 95% credible interval (CrI) estimates were obtained from the posterior distribution of the sum of country-specific estimates to represent the range of possible influenza-associated deaths in a season or year. We calculated influenza-associated deaths for children younger than 5 years for 92 countries with high rates of mortality due to respiratory infection using the same methods.
Findings: EMR-contributing countries represented 57% of the global population. The estimated mean annual influenza-associated respiratory EMR ranged from 0·1 to 6·4 per 100 000 individuals for people younger than 65 years, 2·9 to 44·0 per 100 000 individuals for people aged between 65 and 74 years, and 17·9 to 223·5 per 100 000 for people older than 75 years. We estimated that 291 243-645 832 seasonal influenza-associated respiratory deaths (4·0-8·8 per 100 000 individuals) occur annually. The highest mortality rates were estimated in sub-Saharan Africa (2·8-16·5 per 100 000 individuals), southeast Asia (3·5-9·2 per 100 000 individuals), and among people aged 75 years or older (51·3-99·4 per 100 000 individuals). For 92 countries, we estimated that among children younger than 5 years, 9243-105 690 influenza-associated respiratory deaths occur annually.
Interpretation: These global influenza-associated respiratory mortality estimates are higher than previously reported, suggesting that previous estimates might have underestimated disease burden. The contribution of non-respiratory causes of death to global influenza-associated mortality should be investigated.
Funding: None.
Copyright © 2018 Elsevier Ltd. All rights reserved.
Conflict of interest statement
CC reports grants from the US Centers for Disease Control and Prevention during the conduct of the study, and grants from Sanofi Pasteur, and travel expenses paid for by Parexel, outside the submitted work. BJC reports grants from the National Institute of Allergy and Infectious Diseases, the Health and Medical Research Fund of Hong Kong, Harvard Center for Communicable Disease Dynamics, the National Institute of General Medical Sciences, and the University Grants Committee of Hong Kong, during the conduct of the study; and grants from Sanofi Pasteur, outside the submitted work. JK reports grants from the Foundation for Influenza Epidemiology and travel expenses paid for by the Global Influenza Initiative, outside the submitted work. All other authors declare no competing interests.
Figures

Comment in
-
Challenges in reducing influenza-associated mortality.Lancet. 2018 Mar 31;391(10127):1242-1244. doi: 10.1016/S0140-6736(17)33292-0. Epub 2017 Dec 14. Lancet. 2018. PMID: 29248256 No abstract available.
References
-
- WHO. [accessed May 10, 2016];Influenza (seasonal) fact sheet. 2016 http://www.who.int/mediacentre/factsheets/fs211/en/
-
- UN Population Division. [accessed May 12, 2016];World population prospects. 2017 http://esa.un.org/unpd/wpp/Download/Standard/Population/
