

Interobserver Reliability of the Berlin ARDS Definition and Strategies to Improve the Reliability of ARDS Diagnosis
- PMID: 29248620
- PMCID: PMC5815873
- DOI: 10.1016/j.chest.2017.11.037
Interobserver Reliability of the Berlin ARDS Definition and Strategies to Improve the Reliability of ARDS Diagnosis
Abstract
Background: Failure to reliably diagnose ARDS may be a major driver of negative clinical trials and underrecognition and treatment in clinical practice. We sought to examine the interobserver reliability of the Berlin ARDS definition and examine strategies for improving the reliability of ARDS diagnosis.
Methods: Two hundred five patients with hypoxic respiratory failure from four ICUs were reviewed independently by three clinicians, who evaluated whether patients had ARDS, the diagnostic confidence of the reviewers, whether patients met individual ARDS criteria, and the time when criteria were met.
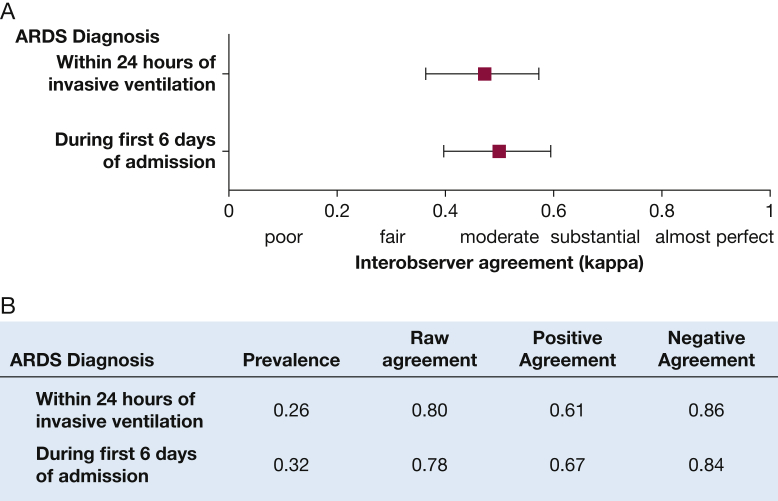
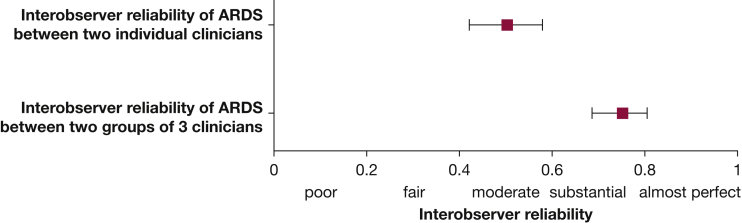
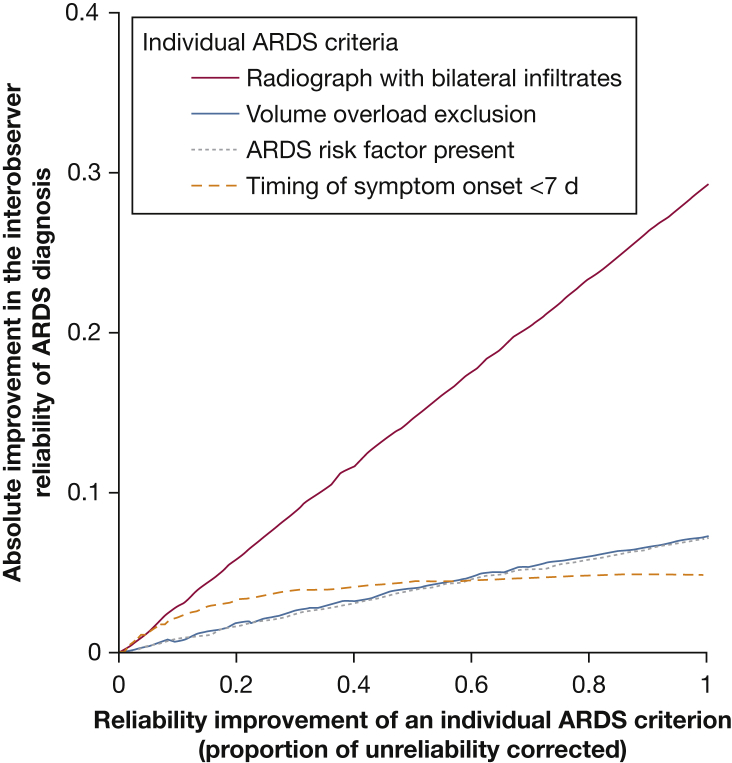
Results: Interobserver reliability of an ARDS diagnosis was "moderate" (kappa = 0.50; 95% CI, 0.40-0.59). Sixty-seven percent of diagnostic disagreements between clinicians reviewing the same patient was explained by differences in how chest imaging studies were interpreted, with other ARDS criteria contributing less (identification of ARDS risk factor, 15%; cardiac edema/volume overload exclusion, 7%). Combining the independent reviews of three clinicians can increase reliability to "substantial" (kappa = 0.75; 95% CI, 0.68-0.80). When a clinician diagnosed ARDS with "high confidence," all other clinicians agreed with the diagnosis in 72% of reviews. There was close agreement between clinicians about the time when a patient met all ARDS criteria if ARDS developed within the first 48 hours of hospitalization (median difference, 5 hours).
Conclusions: The reliability of the Berlin ARDS definition is moderate, driven primarily by differences in chest imaging interpretation. Combining independent reviews by multiple clinicians or improving methods to identify bilateral infiltrates on chest imaging are important strategies for improving the reliability of ARDS diagnosis.
Keywords: ARDS; acute lung injury; clinical trials; diagnosis.
Copyright © 2017 American College of Chest Physicians. All rights reserved.
Figures

Comment in
-
ARDS Cannot Be Accurately Differentiated From Cardiogenic Pulmonary Edema Without Systematic Tissue Doppler Echocardiography.Chest. 2018 Jul;154(1):226-227. doi: 10.1016/j.chest.2018.03.036. Chest. 2018. PMID: 30044739 No abstract available.
-
Response.Chest. 2018 Jul;154(1):227-228. doi: 10.1016/j.chest.2018.03.037. Chest. 2018. PMID: 30044740 No abstract available.
References
-
- Coggon D., Martyn C., Palmer K.T., Evanoff B. Assessing case definitions in the absence of a diagnostic gold standard. Int J Epidemiol. 2005;34(4):949–952. - PubMed
-
- Rubenfeld G.D. Confronting the frustrations of negative clinical trials in acute respiratory distress syndrome. Ann Thorac Surg. 2015;12(suppl 1):S58–S63. - PubMed
-
- Frohlich S., Murphy N., Boylan J.F. ARDS: progress unlikely with non-biological definition. Br J Anaesth. 2013;111(5):696–699. - PubMed
-
- Pham T., Rubenfeld G.D. Fifty years of research in ARDS: the epidemiology of acute respiratory distress syndrome. A 50th birthday review. Am J Respir Crit Care Med. 2017;195(7):860–870. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Miscellaneous
