

Adjunctive rifampicin for Staphylococcus aureus bacteraemia (ARREST): a multicentre, randomised, double-blind, placebo-controlled trial
- PMID: 29249276
- PMCID: PMC5820409
- DOI: 10.1016/S0140-6736(17)32456-X
Adjunctive rifampicin for Staphylococcus aureus bacteraemia (ARREST): a multicentre, randomised, double-blind, placebo-controlled trial
Abstract
Background: Staphylococcus aureus bacteraemia is a common cause of severe community-acquired and hospital-acquired infection worldwide. We tested the hypothesis that adjunctive rifampicin would reduce bacteriologically confirmed treatment failure or disease recurrence, or death, by enhancing early S aureus killing, sterilising infected foci and blood faster, and reducing risks of dissemination and metastatic infection.
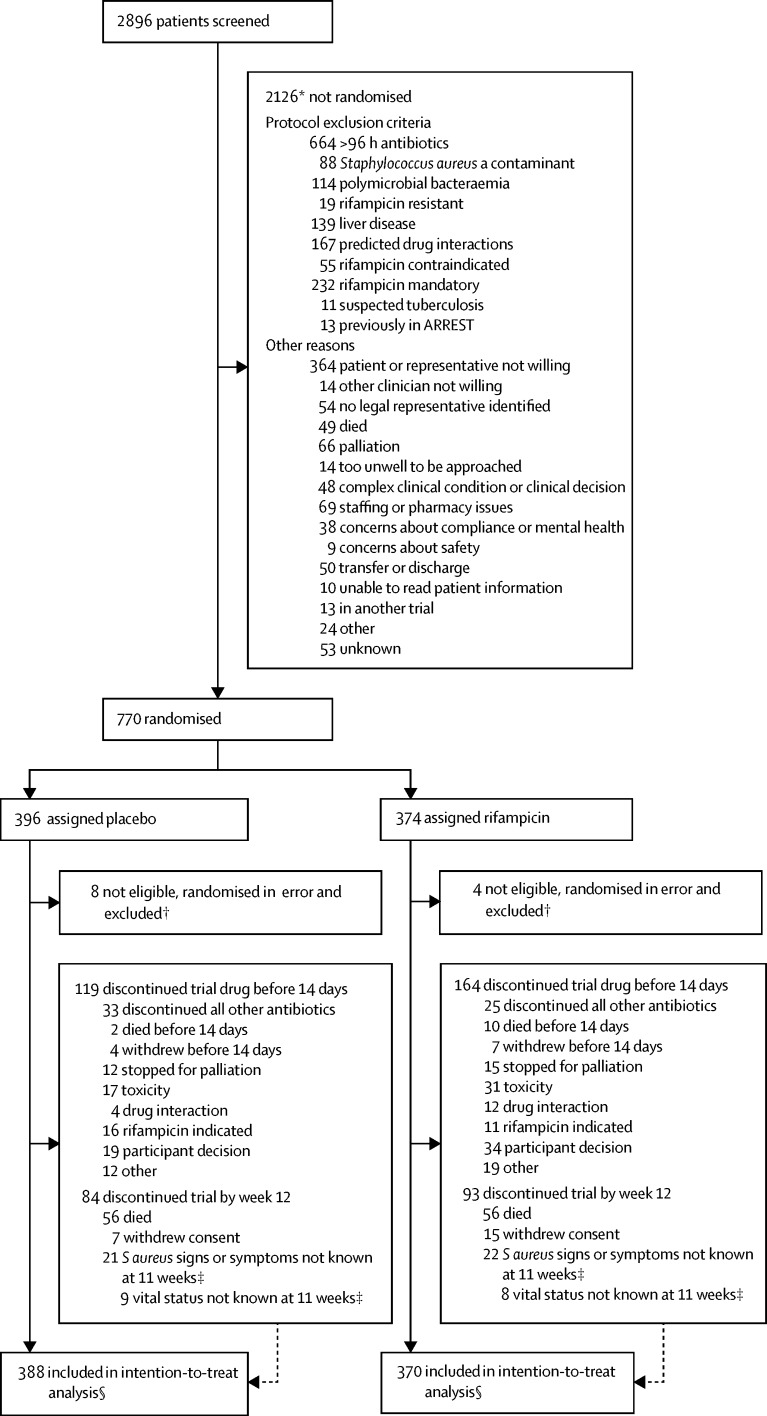
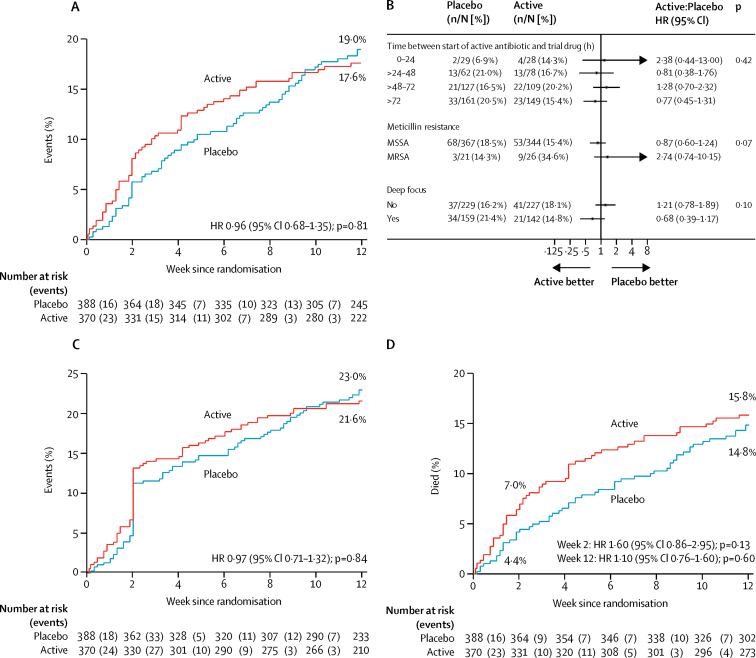
Methods: In this multicentre, randomised, double-blind, placebo-controlled trial, adults (≥18 years) with S aureus bacteraemia who had received ≤96 h of active antibiotic therapy were recruited from 29 UK hospitals. Patients were randomly assigned (1:1) via a computer-generated sequential randomisation list to receive 2 weeks of adjunctive rifampicin (600 mg or 900 mg per day according to weight, oral or intravenous) versus identical placebo, together with standard antibiotic therapy. Randomisation was stratified by centre. Patients, investigators, and those caring for the patients were masked to group allocation. The primary outcome was time to bacteriologically confirmed treatment failure or disease recurrence, or death (all-cause), from randomisation to 12 weeks, adjudicated by an independent review committee masked to the treatment. Analysis was intention to treat. This trial was registered, number ISRCTN37666216, and is closed to new participants.
Findings: Between Dec 10, 2012, and Oct 25, 2016, 758 eligible participants were randomly assigned: 370 to rifampicin and 388 to placebo. 485 (64%) participants had community-acquired S aureus infections, and 132 (17%) had nosocomial S aureus infections. 47 (6%) had meticillin-resistant infections. 301 (40%) participants had an initial deep infection focus. Standard antibiotics were given for 29 (IQR 18-45) days; 619 (82%) participants received flucloxacillin. By week 12, 62 (17%) of participants who received rifampicin versus 71 (18%) who received placebo experienced treatment failure or disease recurrence, or died (absolute risk difference -1·4%, 95% CI -7·0 to 4·3; hazard ratio 0·96, 0·68-1·35, p=0·81). From randomisation to 12 weeks, no evidence of differences in serious (p=0·17) or grade 3-4 (p=0·36) adverse events were observed; however, 63 (17%) participants in the rifampicin group versus 39 (10%) in the placebo group had antibiotic or trial drug-modifying adverse events (p=0·004), and 24 (6%) versus six (2%) had drug interactions (p=0·0005).
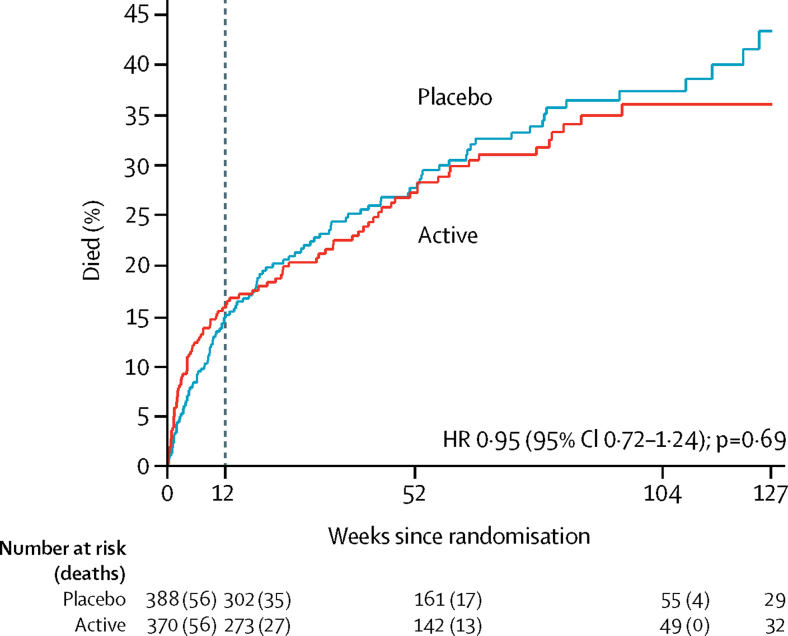
Interpretation: Adjunctive rifampicin provided no overall benefit over standard antibiotic therapy in adults with S aureus bacteraemia.
Funding: UK National Institute for Health Research Health Technology Assessment.
Copyright © 2018 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
Rifampicin for Staphylococcus aureus bacteraemia: give it ARREST.Lancet. 2018 Feb 17;391(10121):634-636. doi: 10.1016/S0140-6736(17)33294-4. Epub 2017 Dec 14. Lancet. 2018. PMID: 29249277 No abstract available.
-
In adults with S aureus bacteremia, adding rifampin to standard antibiotic therapy did not improve outcomes.Ann Intern Med. 2018 Mar 20;168(6):JC32. doi: 10.7326/ACPJC-2018-168-6-032. Ann Intern Med. 2018. PMID: 29554670 No abstract available.
-
Rifampicin in treating S aureus bacteraemia.Lancet. 2018 Aug 18;392(10147):554-555. doi: 10.1016/S0140-6736(18)31555-1. Epub 2018 Aug 16. Lancet. 2018. PMID: 30152387 No abstract available.
-
Rifampicin in treating S aureus bacteraemia - Authors' reply.Lancet. 2018 Aug 18;392(10147):555-556. doi: 10.1016/S0140-6736(18)31545-9. Epub 2018 Aug 16. Lancet. 2018. PMID: 30152388 No abstract available.
References
-
- Thwaites GE, Edgeworth JD, Gkrania-Klotsas E. Clinical management of Staphylococcus aureus bacteraemia. Lancet Infect Dis. 2011;11:208–222. - PubMed
-
- Naber CK, Baddour LM, Giamarellos-Bourboulis EJ. Clinical consensus conference: survey on Gram-positive bloodstream infections with a focus on Staphylococcus aureus. Clin Infect Dis. 2009;48(suppl 4):S260–S270. - PubMed
-
- Liu C, Bayer A, Cosgrove SE. Clinical practice guidelines by the Infectious Diseases Society of America for the treatment of methicillin-resistant Staphylococcus aureus infections in adults and children. Clin Infect Dis. 2011;52:e18–e55. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
