

Benchmarking clinical outcomes and the immunocatabolic phenotype of chronic critical illness after sepsis in surgical intensive care unit patients
- PMID: 29251709
- PMCID: PMC5780256
- DOI: 10.1097/TA.0000000000001758
Benchmarking clinical outcomes and the immunocatabolic phenotype of chronic critical illness after sepsis in surgical intensive care unit patients
Abstract
Background: A growing number of patients survive sepsis but remain chronically critically ill. We sought to define clinical outcomes and incidence of chronic critical illness (CCI) after sepsis and to determine whether selected biomarkers of inflammation, immunosuppression, and catabolism differ between these patients and those that rapidly recover (RAP).
Methods: This 3-year prospective observational cohort study (NCT02276417) evaluated 145 surgical intensive care unit patients with sepsis for the development of CCI (≥14 days of intensive care unit resource utilization with persistent organ dysfunction). Patient clinical demographics, outcomes, and serial serum/urine samples were collected for plasma protein and urinary metabolite analyses.
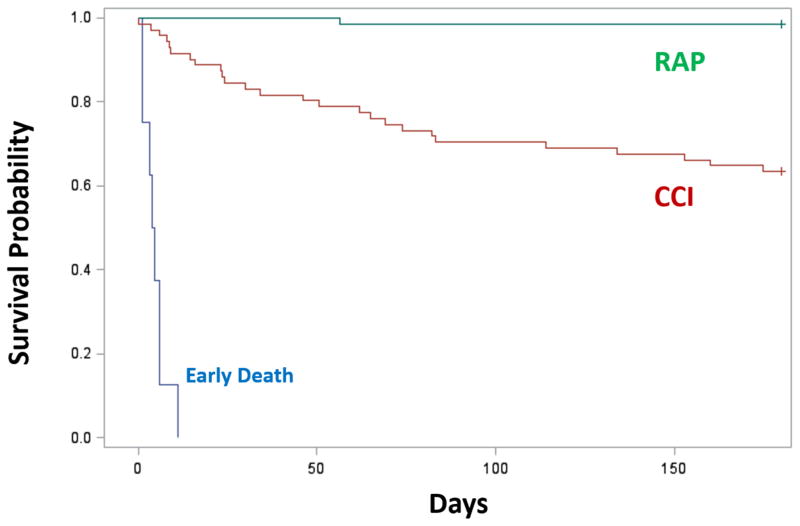
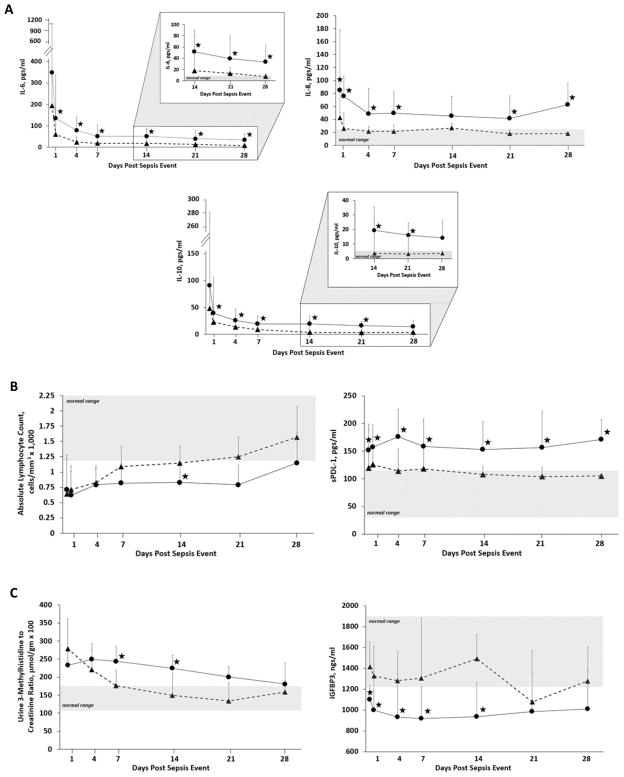
Results: Of 145 sepsis patients enrolled, 19 (13%) died during their hospitalization and 71 (49%) developed CCI. The CCI patients were significantly older (mean, 63 ± 15 vs. 58 ± 13 years, p = 0.006) and more likely to be discharged to long-term acute care facilities (32% vs. 3%, p < 0.0001), whereas those with RAP were more often discharged to home or a rehabilitation facility. Six-month mortality was significantly higher in CCI as compared with RAP cohort (37% vs. 2%; p < 0.01). Multivariate logistic regression modeling revealed delayed onset sepsis (>48 hours after admission; odds ratio [OR], 10.93; 95% confidence interval [CI], 4.15-28.82]), interfacility transfer (OR, 3.58; 95% CI, 1.43-8.96), vasopressor-dependent septic shock (OR, 3.75; 95% CI, 1.47-9.54), and Sequential Organ Failure Assessment score of 5 or greater at 72 hours (OR, 5.03; 95% CI, 2.00-12.62) as independent risk factors for the development of CCI. The CCI patients also demonstrated greater elevations in inflammatory cytokines (IL-6, IL-8, IL-10), and biomarker profiles are consistent with persistent immunosuppression (absolute lymphocyte count and soluble programmed death ligand 1) and catabolism (plasma insulin-like growth factor binding protein 3 and urinary 3-methylhistidine excretion).
Conclusion: The development of CCI has become the predominant clinical trajectory in critically ill surgical patients with sepsis. These patients exhibit biomarker profiles consistent with an immunocatabolic phenotype of persistent inflammation, immunosuppression, and catabolism.
Level of evidence: Prognostic, level II.
Figures
References
-
- Kaukonen KM, Bailey M, Suzuki S, Pilcher D, Bellomo R. Mortality related to severe sepsis and septic shock among critically ill patients in Australia and New Zealand, 2000–2012. JAMA. 2014;311(13):1308–16. - PubMed
-
- Moore LJ, McKinley BA, Turner KL, Todd SR, Sucher JF, Valdivia A, Sailors RM, Kao LS, Moore FA. The epidemiology of sepsis in general surgery patients. J Trauma. 2011;70(3):672–80. - PubMed
-
- Levy MM, Dellinger RP, Townsend SR, Linde-Zwirble WT, Marshall JC, Bion J, Schorr C, Artigas A, Ramsay G, Beale R, et al. The Surviving Sepsis Campaign: results of an international guideline-based performance improvement program targeting severe sepsis. Intensive Care Med. 2010;36(2):222–31. - PMC - PubMed
-
- Levy MM, Rhodes A, Phillips GS, Townsend SR, Schorr CA, Beale R, Osborn T, Lemeshow S, Chiche JD, Artigas A, et al. Surviving Sepsis Campaign: association between performance metrics and outcomes in a 7.5-year study. Crit Care Med. 2015;43(1):3–12. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
