

Pertuzumab, trastuzumab, and standard anthracycline- and taxane-based chemotherapy for the neoadjuvant treatment of patients with HER2-positive localized breast cancer (BERENICE): a phase II, open-label, multicenter, multinational cardiac safety study
- PMID: 29253081
- PMCID: PMC5888999
- DOI: 10.1093/annonc/mdx773
Pertuzumab, trastuzumab, and standard anthracycline- and taxane-based chemotherapy for the neoadjuvant treatment of patients with HER2-positive localized breast cancer (BERENICE): a phase II, open-label, multicenter, multinational cardiac safety study
Abstract
Background: Anti-HER2 therapies are associated with a risk of increased cardiac toxicity, particularly when part of anthracycline-containing regimens. We report cardiac safety of pertuzumab, trastuzumab, and chemotherapy in the neoadjuvant treatment of HER2-positive early breast cancer.
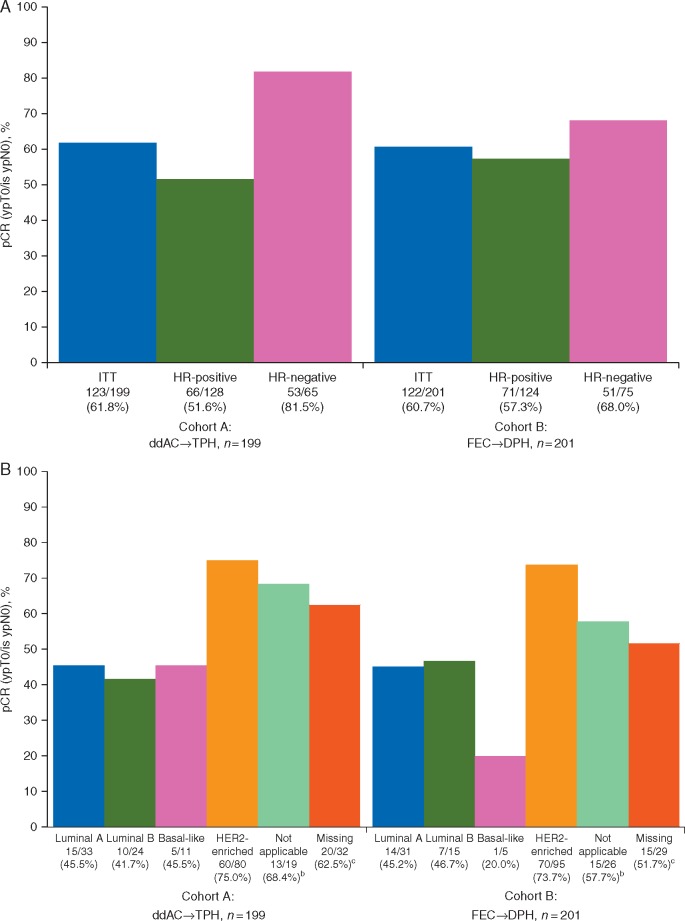
Patients and methods: BERENICE (NCT02132949) is a nonrandomized, phase II, open-label, multicenter, multinational study in patients with normal cardiac function. In the neoadjuvant period, cohort A patients received four cycles of dose-dense doxorubicin and cyclophosphamide, then 12 doses of standard paclitaxel plus four standard trastuzumab and pertuzumab cycles. Cohort B patients received four standard fluorouracil/epirubicin/cyclophosphamide cycles, then four docetaxel cycles with four standard trastuzumab and pertuzumab cycles. The primary end point was cardiac safety during neoadjuvant treatment, assessed by the incidence of New York Heart Association class III/IV heart failure and of left ventricular ejection fraction declines (≥10 percentage-points from baseline and to a value of <50%). The main efficacy end point was pathologic complete response (pCR, ypT0/is ypN0). Results are descriptive.
Results: Safety populations were 199 and 198 patients in cohorts A and B, respectively. Three patients [1.5%; 95% confidence interval (CI) 0.31% to 4.34%] in cohort A experienced four New York Heart Association class III/IV heart failure events. Thirteen patients (6.5%; 95% CI 3.5% to 10.9%) in cohort A and four (2.0%; 95% CI 0.6% to 5.1%) in cohort B experienced at least one left ventricular ejection fraction decline. No new safety signals were identified. pCR rates were 61.8% and 60.7% in cohorts A and B, respectively. The highest pCR rates were in the HER2-enriched PAM50 subtype (75.0% and 73.7%, respectively).
Conclusion: Treatment with pertuzumab, trastuzumab, and common anthracycline-containing regimens for the neoadjuvant treatment of early breast cancer resulted in cardiac and general safety profiles, and pCR rates, consistent with prior studies with pertuzumab.
Clinical trial information: NCT02132949.
Figures

References
-
- Wolff AC, Hammond ME, Hicks DG. et al. Recommendations for human epidermal growth factor receptor 2 testing in breast cancer: American Society of Clinical Oncology/College of American Pathologists clinical practice guideline update. J Clin Oncol 2013; 31(31): 3997–4013. - PubMed
-
- Slamon DJ, Leyland-Jones B, Shak S. et al. Use of chemotherapy plus a monoclonal antibody against HER2 for metastatic breast cancer that overexpresses HER2. N Engl J Med 2001; 344(11): 783–792. - PubMed
-
- Gianni L, Pienkowski T, Im YH. et al. Efficacy and safety of neoadjuvant pertuzumab and trastuzumab in women with locally advanced, inflammatory, or early HER2-positive breast cancer (NeoSphere): a randomised multicentre, open-label, phase 2 trial. Lancet Oncol 2012; 13(1): 25–32. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
