

Addition of Estradiol to Cross-Sex Testosterone Therapy Reduces Atherosclerosis Plaque Formation in Female ApoE-/- Mice
- PMID: 29253190
- PMCID: PMC5774248
- DOI: 10.1210/en.2017-00884
Addition of Estradiol to Cross-Sex Testosterone Therapy Reduces Atherosclerosis Plaque Formation in Female ApoE-/- Mice
Abstract
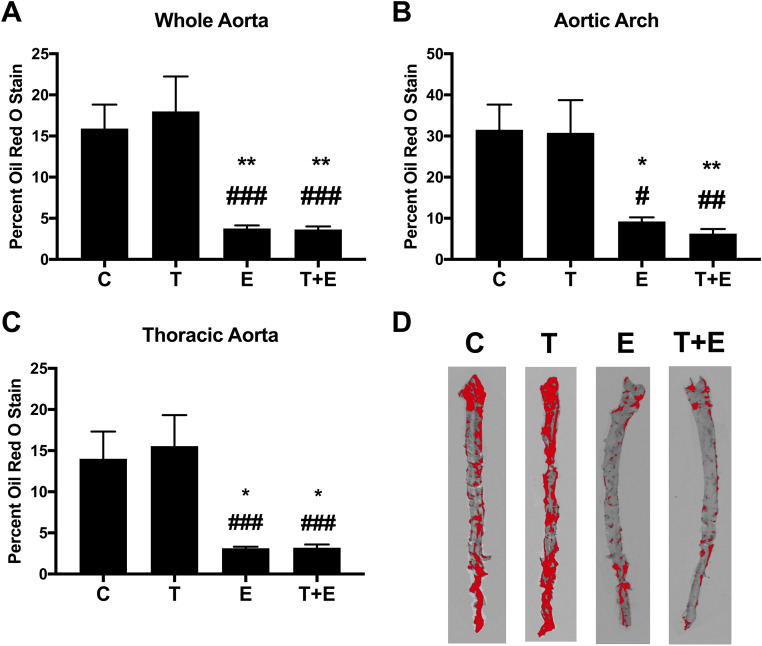
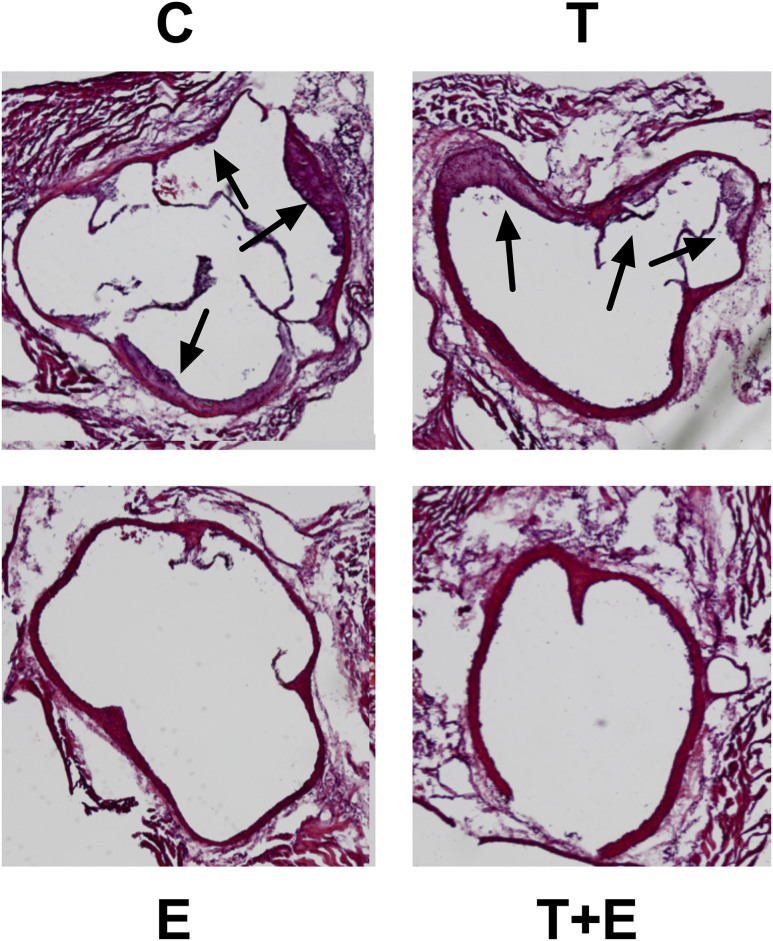
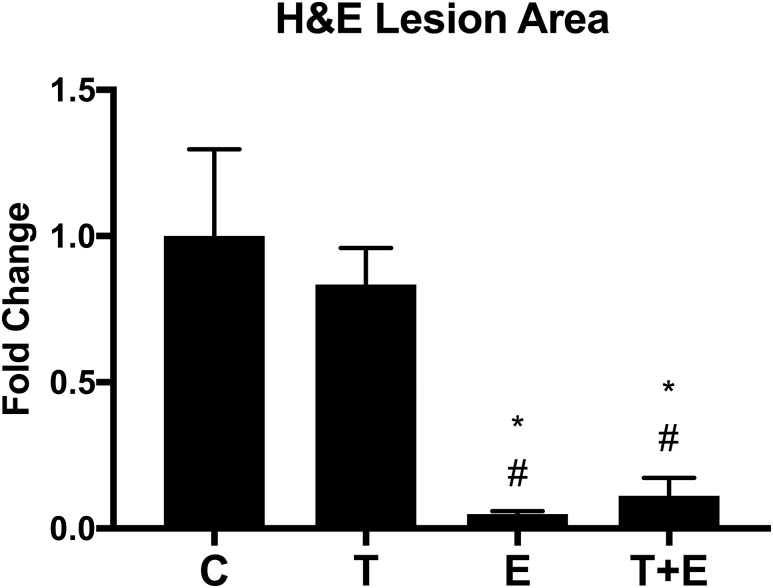
The contributions of estradiol and testosterone to atherosclerotic lesion progression are not entirely understood. Cross-sex hormone therapy (XHT) for transgender individuals dramatically alters estrogen and testosterone levels and consequently could have widespread consequences for cardiovascular health. Yet, no preclinical research has assessed atherosclerosis risk after XHT. We examined the effects of testosterone XHT after ovariectomy on atherosclerosis plaque formation in female mice and evaluated whether adding low-dose estradiol to cross-sex testosterone treatments after ovariectomy reduced lesion formation. Six-week-old female ApoE-/- C57BL/6 mice underwent ovariectomy and began treatments with testosterone, estradiol, testosterone with low-dose estradiol, or vehicle alone until euthanized at 23 weeks of age. Atherosclerosis lesion progression was measured by Oil Red O stain and confirmed histologically. We found reduced atherosclerosis in the estradiol- and combined testosterone/estradiol-treated mice compared with those treated with testosterone or vehicle only in the whole aorta (-75%), aortic arch (-80%), and thoracic aorta (-80%). Plaque size was similarly reduced in the aortic sinus. These reductions in lesion size after combined testosterone/estradiol treatment were comparable to those obtained with estrogen alone. Testosterone/estradiol combined therapy resulted in less atherosclerosis plaque formation than either vehicle or testosterone alone after ovariectomy. Testosterone/estradiol therapy was comparable to estradiol replacement alone, whereas mice treated with testosterone only fared no better than untreated controls after ovariectomy. Adding low-dose estrogen to cross-sex testosterone therapy after oophorectomy could improve cardiovascular outcomes for transgender patients. Additionally, these results contribute to understanding of the effects of estrogen and testosterone on atherosclerosis progression.
Copyright © 2018 Endocrine Society.
Figures
References
-
- Flores AR, Herman JL, Gates GJ, Brown TN. How Many Adults Identify as Transgender in the United States. Los Angeles, CA: The Williams Institute; 2016.
-
- Hembree WC, Cohen-Kettenis P, Delemarre-van de Waal HA, Gooren LJ, Meyer WJ III, Spack NP, Tangpricha V, Montori VM; Endocrine Society . Endocrine treatment of transsexual persons: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2009;94(9):3132–3154. - PubMed
-
- Kailas M, Lu HMS, Rothman EF, Safer JD. Prevalence and types of gender-affirming surgery among a sample of transgender endocrinology patients prior to state expansion of insurance coverage. Endocr Pract. 2017;23(7):780–786. - PubMed
-
- Wierckx K, Elaut E, Declercq E, Heylens G, De Cuypere G, Taes Y, Kaufman JM, T’Sjoen G. Prevalence of cardiovascular disease and cancer during cross-sex hormone therapy in a large cohort of trans persons: a case-control study. Eur J Endocrinol. 2013;169(4):471–478. - PubMed
-
- Wierckx K, Mueller S, Weyers S, Van Caenegem E, Roef G, Heylens G, T’Sjoen G. Long-term evaluation of cross-sex hormone treatment in transsexual persons. J Sex Med. 2012;9(10):2641–2651. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Miscellaneous
