

Acute myocardial infarction hospital admissions and deaths in England: a national follow-back and follow-forward record-linkage study
- PMID: 29253451
- PMCID: PMC6196770
- DOI: 10.1016/S2468-2667(17)30032-4
Acute myocardial infarction hospital admissions and deaths in England: a national follow-back and follow-forward record-linkage study
Abstract
Background: Little information is available on how primary and comorbid acute myocardial infarction contribute to the mortality burden of acute myocardial infarction, the share of these deaths that occur during or after a hospital admission, and the reasons for hospital admission of those who died from acute myocardial infarction. Our aim was to fill in these gaps in the knowledge about deaths and hospital admissions due to acute myocardial infarction.
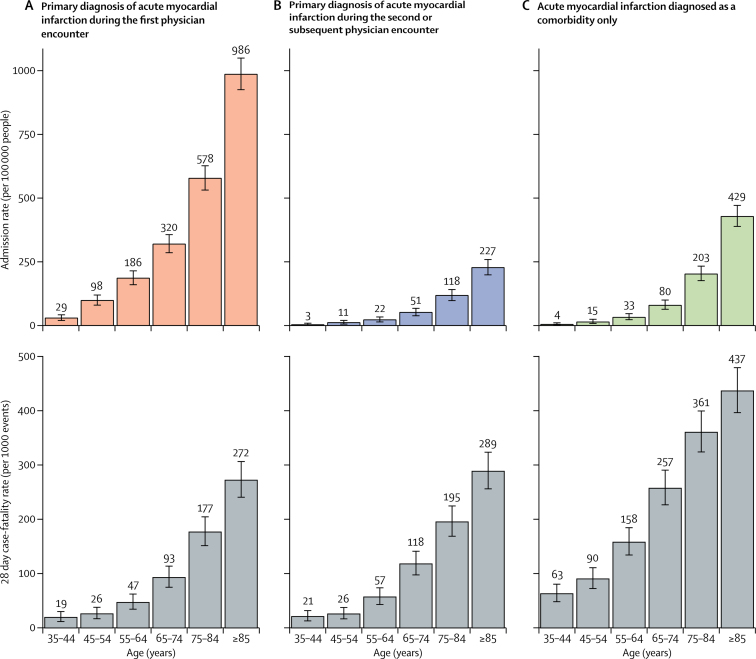
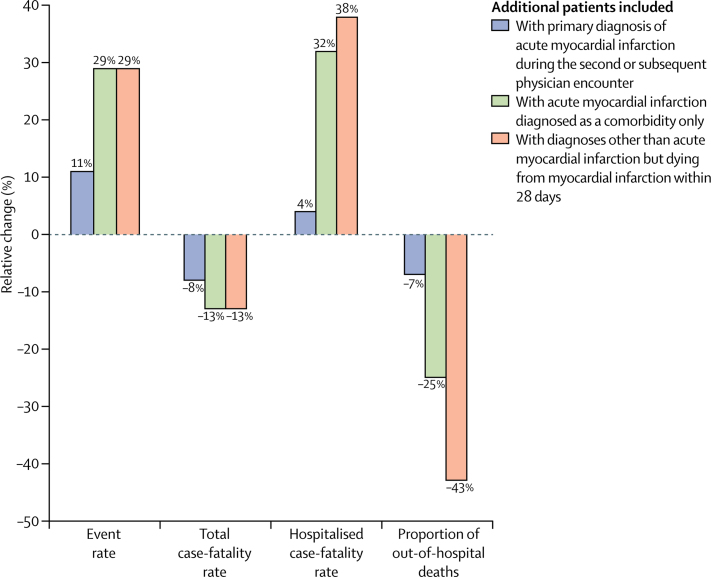
Methods: We used individually linked national hospital admission and mortality data for England from 2006 to 2010 to identify all primary and comorbid diagnoses of acute myocardial infarction during hospital stay and their associated fatality rates (during or within 28 days of being in hospital). Data were obtained from the UK Small Area Health Statistics Unit and supplied by the Health and Social Care Information Centre (now NHS Digital) and the Office of National Statistics. We calculated event rates (reported as per 100 000 population for relevant age and sex groups) and case-fatality rate for primary acute myocardial infarction diagnosed during the first physician encounter or during subsequent encounters, and acute myocardial infarction diagnosed only as a comorbidity. We also calculated what proportion of deaths from acute myocardial infarction occurred in people who had been in hospital on or within the 28 days preceding death, and whether acute myocardial infarction was one of the recorded diagnoses in such admissions.
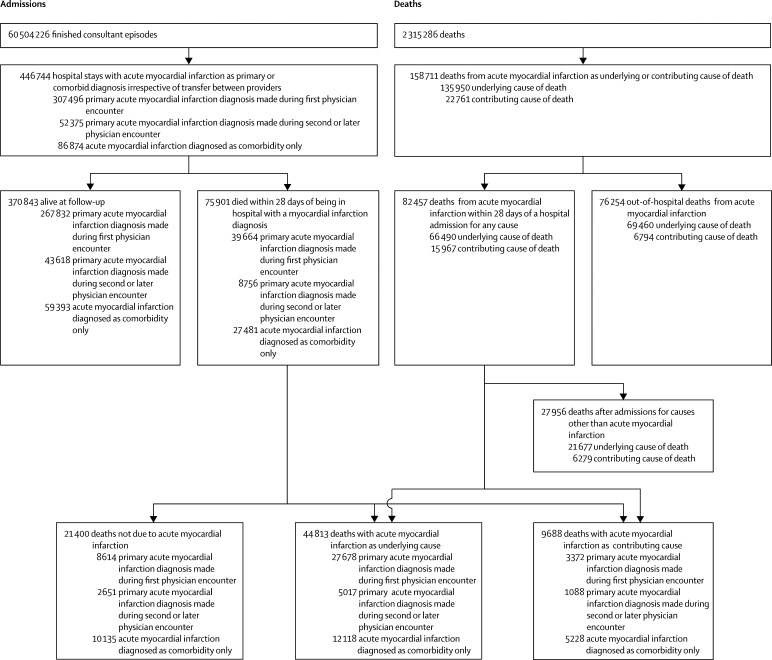
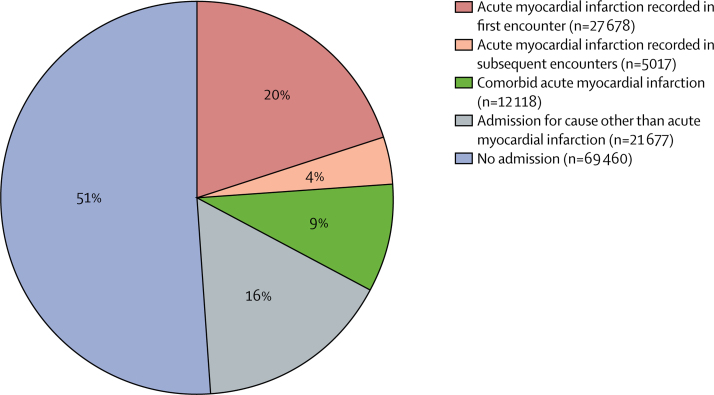
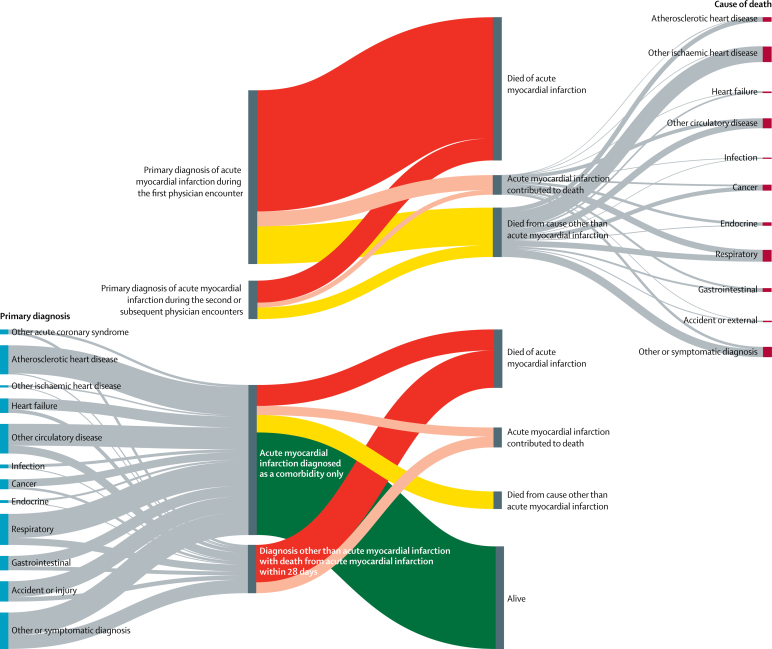
Findings: Acute myocardial infarction was diagnosed in the first physician encounter in 307 496 (69%) of 446 744 admissions with a diagnosis of acute myocardial infarction, in the second or later physician encounter in 52 374 (12%) admissions, and recorded only as a comorbidity in 86 874 (19%) admissions. Patients with comorbid diagnoses of acute myocardial infarction had two to three times the case-fatality rate of patients in whom acute myocardial infarction was a primary diagnosis. 135 950 deaths were recorded as being caused by acute myocardial infarction as the underlying cause of death, of which 66 490 (49%) occurred in patients who were in hospital on the day of death or in the 28 days preceding death. AMI was the primary diagnosis in 32 695 (49%) of these 66 490 patients (27 678 [42%] diagnosed in the first physician encounter and 5017 [8%] in a second or subsequent encounter), was a comorbid diagnosis in 12 118 (18%), and was not mentioned at all in the remaining 21 677 (33%). The most common causes of admission in people who did not have an acute myocardial infarction diagnosis but went on to die of acute myocardial infarction as the underlying cause of death were other circulatory conditions (7566 [35%] of 21 677 deaths), symptomatic diagnoses including non-specific chest pain, dyspnoea and syncope (1368 [6%] deaths), and respiratory disorders (2662 [12%] deaths), mainly pneumonia and chronic obstructive airways disease.
Interpretation: As many acute myocardial infarction deaths occurring within 28 days of being in hospital follow a non-acute myocardial infarction admission as follow an acute myocardial infarction admission. These people are often diagnosed with other circulatory disorders or symptoms of circulatory disturbance. Further investigation is needed to establish whether there are symptoms and information that can be used to predict the risk of a fatal acute myocardial infarction in such patients, which can contribute to reducing the mortality burden of acute myocardial infarction.
Funding: Wellcome Trust, Medical Research Council, Public Health England, National Institute for Health Research.
Copyright © 2017 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY license. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
Record-linkage studies: dates and event-definitions matter hugely.Lancet Public Health. 2017 Apr;2(4):e164. doi: 10.1016/S2468-2667(17)30044-0. Epub 2017 Mar 1. Lancet Public Health. 2017. PMID: 29253446 Free PMC article. No abstract available.
References
-
- Barnett K, Mercer SW, Norbury M, Watt G, Wyke S, Guthrie B. Epidemiology of multimorbidity and implications for health care, research, and medical education: a cross-sectional study. Lancet. 2012;380:37–43. - PubMed
-
- Fox CS, Evans JC, Larson MG, Kannel WB, Levy D. Temporal trends in coronary heart disease mortality and sudden cardiac death from 1950 to 1999: the Framingham Heart Study. Circulation. 2004;110:522–527. - PubMed
-
- McGovern PG, Jacobs DR, Jr, Shahar E. Trends in acute coronary heart disease mortality, morbidity, and medical care from 1985 through 1997: the Minnesota heart survey. Circulation. 2001;104:19–24. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
