

Racism and health service utilisation: A systematic review and meta-analysis
- PMID: 29253855
- PMCID: PMC5734775
- DOI: 10.1371/journal.pone.0189900
Racism and health service utilisation: A systematic review and meta-analysis
Abstract
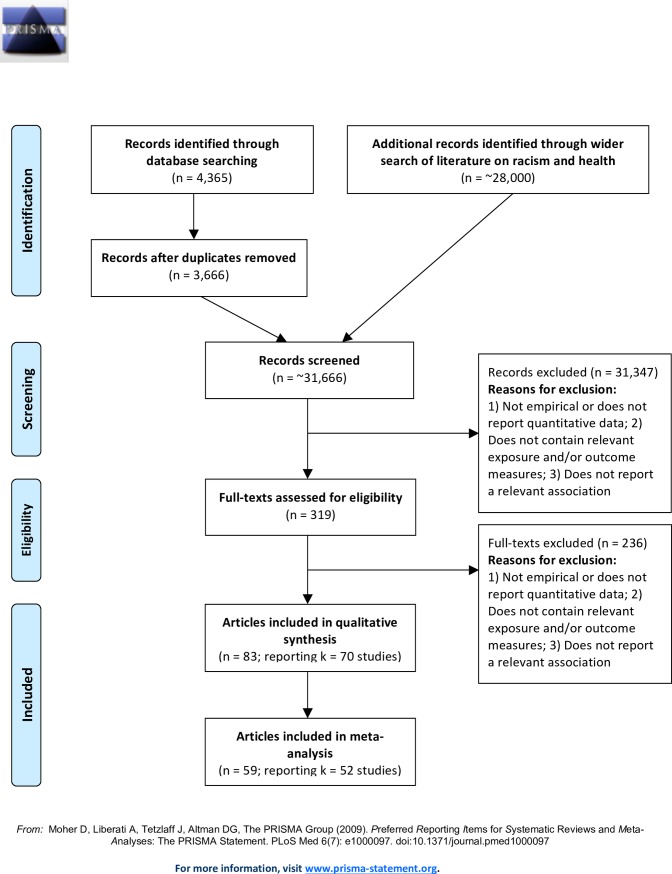
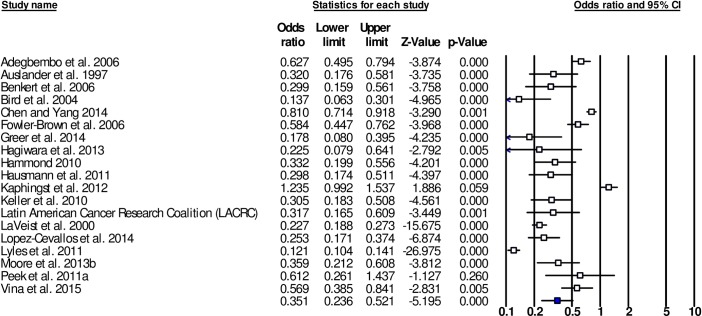
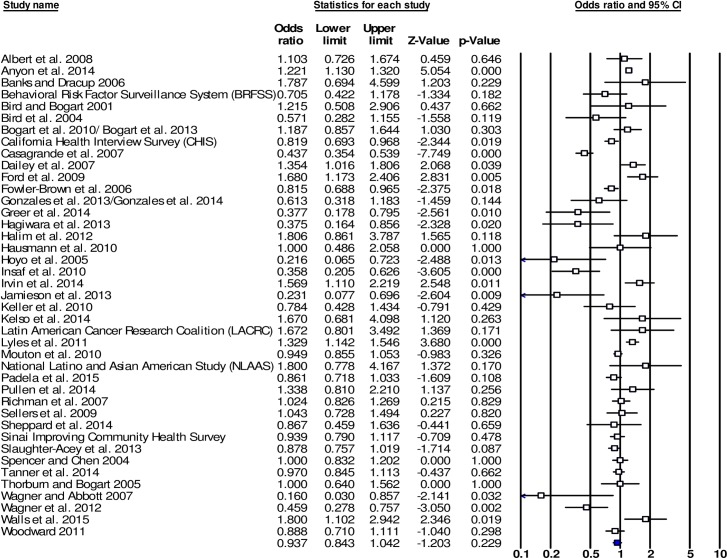
Although racism has been posited as driver of racial/ethnic inequities in healthcare, the relationship between racism and health service use and experience has yet to be systematically reviewed or meta-analysed. This paper presents a systematic review and meta-analysis of quantitative empirical studies that report associations between self-reported racism and various measures of healthcare service utilisation. Data were reviewed and extracted from 83 papers reporting 70 studies. Studies included 250,850 participants and were conducted predominately in the U.S. The meta-analysis included 59 papers reporting 52 studies, which were analysed using random effects models and mean weighted effect sizes. Racism was associated with more negative patient experiences of health services (HSU-E) (OR = 0.351 (95% CI [0.236,0.521], k = 19), including lower levels of healthcare-related trust, satisfaction, and communication. Racism was not associated with health service use (HSU-U) as an outcome group, and was not associated with most individual HSU-U outcomes, including having had examinations, health service visits and admissions to health professionals and services. Racism was associated with health service use outcomes such as delaying/not getting healthcare, and lack of adherence to treatment uptake, although these effects may be influenced by a small sample of studies, and publication bias, respectively. Limitations to the literature reviewed in terms of study designs, sampling methods and measurements are discussed along with suggested future directions in the field.
Conflict of interest statement
Figures
References
-
- Ahmed S, Shommu NS, Rumana N, Barron GR, Wicklum S, Turin TC. Barriers to access of primary healthcare by immigrant populations in Canada: a literature review. Journal of immigrant and minority health. 2016. December 1;18(6):1522–40. doi: 10.1007/s10903-015-0276-z - DOI - PubMed
-
- Brondolo E, Gallo LC, Myers HF. Race, racism and health: disparities, mechanisms, and interventions. Journal of behavioral medicine. 2009. February 1;32(1):1–8. doi: 10.1007/s10865-008-9190-3 - DOI - PubMed
-
- Fiscella K, Sanders MR. Racial and ethnic disparities in the quality of health care. Annual review of public health. 2016. March 18;37:375–94. doi: 10.1146/annurev-publhealth-032315-021439 - DOI - PubMed
-
- Ministry of Health. Tatau kahukura: Māori health chart book 3rd ed Wellington: Ministry of Health; 2015.
-
- Smedley BE, Stith AY, Nelson AR. Unequal treatment: Confronting ethnic and racial disparities in health care. Washington, DC: Institute of Medicine; 2003. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
