

Innovation in endocrine surgery: robotic versus laparoscopic adrenalectomy. Meta-analysis and systematic literature review
- PMID: 29254254
- PMCID: PMC5731964
- DOI: 10.18632/oncotarget.22059
Innovation in endocrine surgery: robotic versus laparoscopic adrenalectomy. Meta-analysis and systematic literature review
Abstract
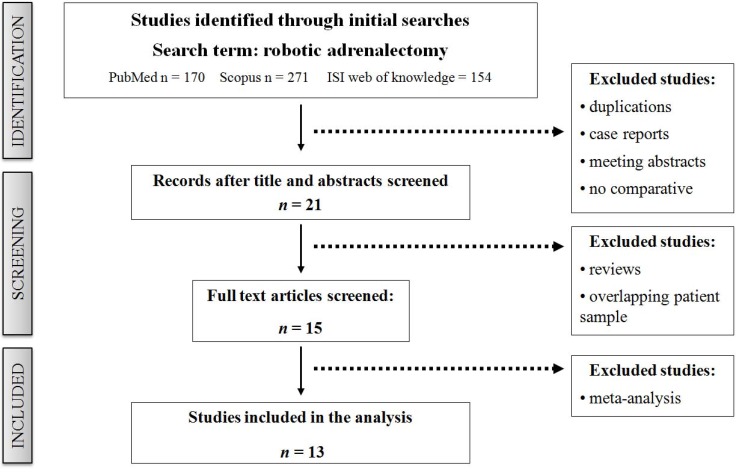
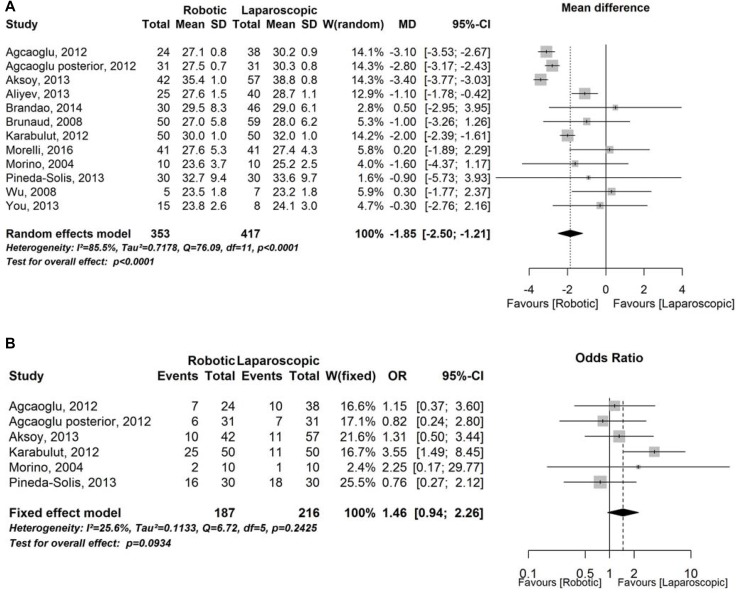
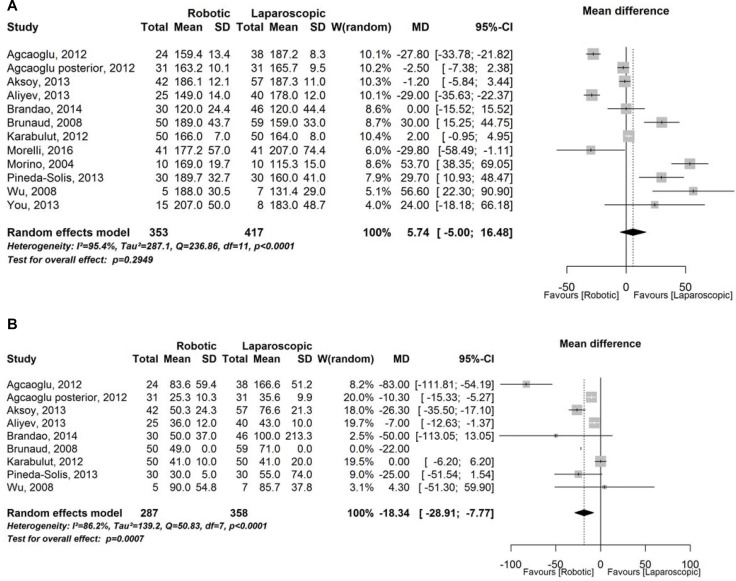
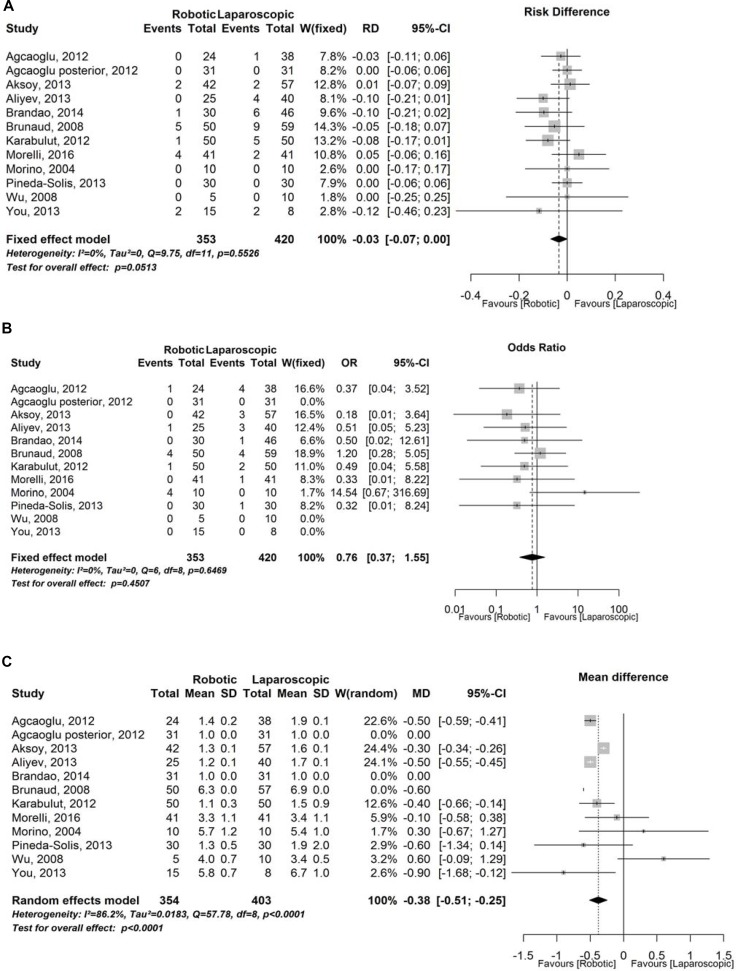
Several studies in the last years demonstrated the better surgical outcome of laparoscopic approach to adrenal gland. Laparoscopic surgery is more difficult to learn and requires different psychomotor skills than open surgery, especially with regard to complex maneuvers requiring precision and dexterity. The development of robotic platform with three-dimensional vision and increased degrees of freedom of the surgical instruments has the aim to overcome these problems. We performed a systematic literature review with meta-analysis to evaluate preoperative data and surgical outcomes of robotic adrenalectomy compared with laparoscopic technique. In September 2016 we performed a systematic literature review using the Pubmed, Scopus and ISI web of knowledge database with search term "robotic adrenalectomy". We identified 13 studies with eligible criteria that compared surgical outcomes. This present systematic review with meta-analysis includes 798 patients: 379 underwent to robotic adrenalectomy (cases group) and 419 to laparoscopic adrenalectomy (controls group). There were no significant differences between the two groups of patients respect to age, gender, laterality and tumor size. BMI instead was significant lower in the robotic group. In this group we found also patients with higher incidence of previous abdominal surgery. The results from operative time demonstrated lower operative time for laparoscopic group but there were no significant differences with robotic group. Robotic adrenalectomy showed a significant lower blood loss. Robotic adrenalectomy is a safe and feasible technique with reduced blood loss and shorter hospital stay than laparoscopic adrenalectomy. Laparoscopic approach seems to be a more rapid technique when comparing to robotic technique, although recent studies demonstrate a significant operative time reduction in robotic group with the learning curve improvement and the development of new surgical technology.
Keywords: adrenal surgery; laparoscopic adrenalectomy; laparoscopic surgery; robotic adrenalectomy; robotic surgery.
Conflict of interest statement
CONFLICTS OF INTEREST None.
Figures
References
-
- Gagner M, Lacroix A, Bolte E. Laparoscopic adrenalectomy in Cushing's syndrome and pheochromocytoma. N Engl J Med. 1992;327:1033. - PubMed
-
- Conzo G, Tartaglia E, Gambardella C, Esposito D, Sciascia V, Mauriello C, Nunziata A, Siciliano G, Izzo G, Cavallo F, Thomas G, Musella M, Santini L. Minimally invasive approach for adrenal lesions: Systematic review of laparoscopic versus retroperitoneoscopic adrenalectomy and assessment of risk factors for complications. Int J Surg. 2016;28:S118–23. https://doi.org/10.1016/j.ijsu.2015.12.042. - DOI - PubMed
-
- Romano G, Agrusa A, Chianetta D, Frazzetta G, Sorce V, Di Buono G, Gulotta G. Laparoscopic management of adrenal tumors: a four-years experience in a single center. Minerva Chir. 2014;69:125–129.
-
- Agrusa A, Romano G, De Vita G, Frazzetta G, Chianetta D, Di Buono G, Gulotta G. Adrenal gunshot wound: Laparoscopic approach. Report of a case. Int J Surg Case Rep. 2014;5:70–2. https://doi.org/10.1016/j.ijscr.2013.12.020. - DOI - PMC - PubMed
-
- Agrusa A, Romano G, Dominguez LJ, Amato G, Citarrella R, Vernuccio L, Di Buono G, Sorce V, Gulotta L, Galia M, Mansueto P, Gulotta G. Adrenal cavernous hemangioma: which correct decision making process? Acta Medica Mediterranea. 2016;32:385–389. https://doi.org/10.19193/0393-6384_2016_2_58. - DOI
LinkOut - more resources
Full Text Sources
Other Literature Sources
