

Myocardial computed tomography perfusion
- PMID: 29255689
- PMCID: PMC5716942
- DOI: 10.21037/cdt.2017.06.11
Myocardial computed tomography perfusion
Abstract
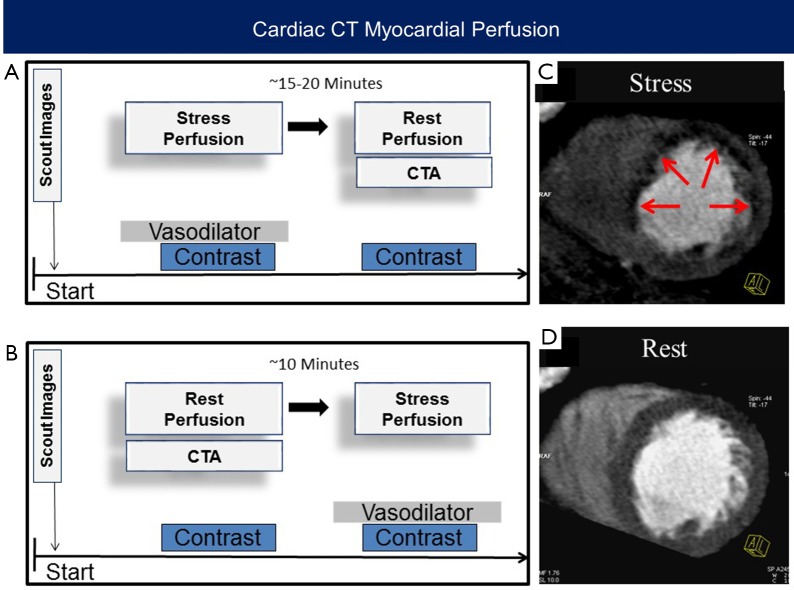
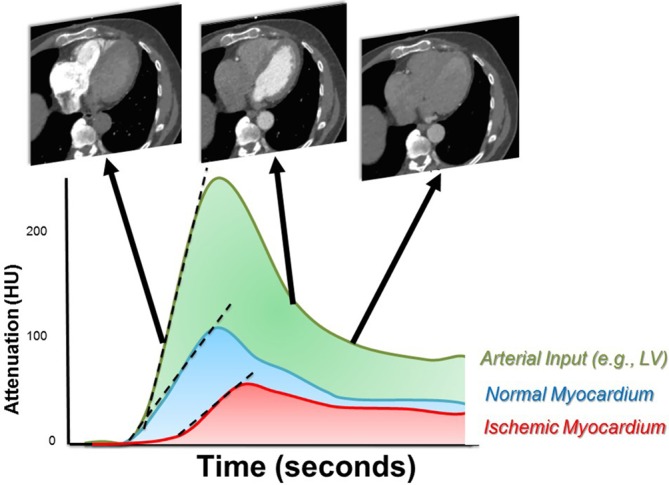
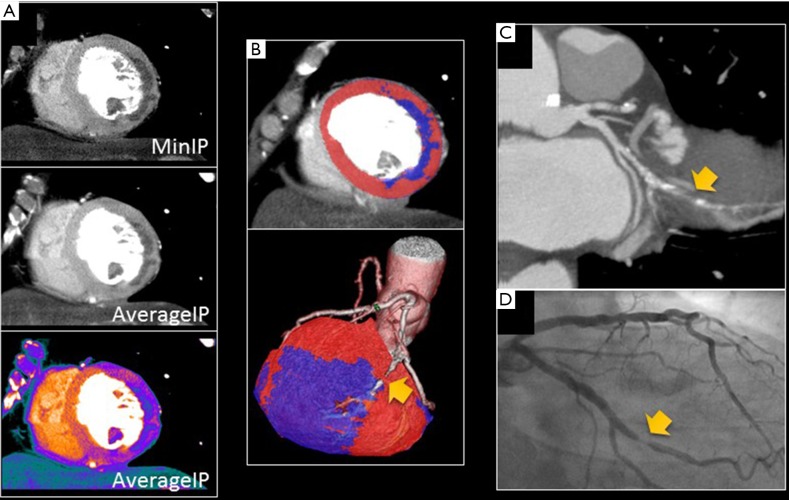
Despite having excellent diagnostic accuracy to detect anatomical coronary stenosis, coronary CT angiography (CTA) has a limited specificity to detect myocardial ischemia. CT perfusion (CTP) can identify myocardial perfusion defects during vasodilator stress, and when added to coronary CTA, improves the specificity of detecting hemodynamically significant stenosis. A CTP protocol typically involves the acquisition of two separate data sets: (I) a rest scan that can be used as both a coronary CTA and for evaluating rest myocardial perfusion, and (II) a stress CTP scan acquired during vasodilator stress testing. This review summarizes some the techniques, strengths, and limitations of CTP, and provides an overview of the recent evidence supporting the potential use of CTP in clinical practice.
Keywords: CT perfusion (CTP); Stress test; cardiac CT; ischemia; myocardial perfusion imaging.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources