

Prognostic accuracy of age-adapted SOFA, SIRS, PELOD-2, and qSOFA for in-hospital mortality among children with suspected infection admitted to the intensive care unit
- PMID: 29256116
- PMCID: PMC5816088
- DOI: 10.1007/s00134-017-5021-8
Prognostic accuracy of age-adapted SOFA, SIRS, PELOD-2, and qSOFA for in-hospital mortality among children with suspected infection admitted to the intensive care unit
Abstract
Purpose: The Sepsis-3 consensus task force defined sepsis as life-threatening organ dysfunction caused by dysregulated host response to infection. However, the clinical criteria for this definition were neither designed for nor validated in children. We validated the performance of SIRS, age-adapted SOFA, quick SOFA and PELOD-2 scores as predictors of outcome in children.
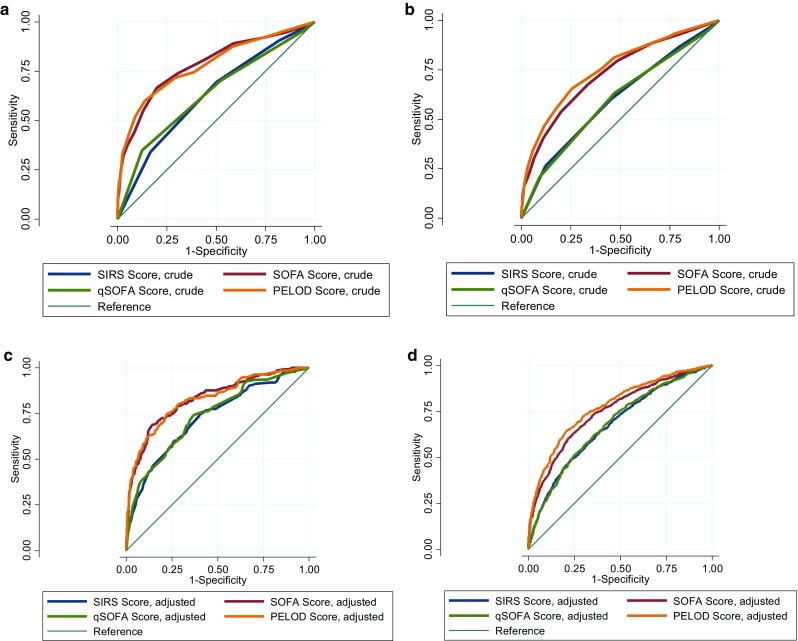
Methods: We performed a multicentre binational cohort study of patients < 18 years admitted with infection to ICUs in Australia and New Zealand. The primary outcome was ICU mortality. SIRS, age-adapted SOFA, quick SOFA and PELOD-2 scores were compared using crude and adjusted area under the receiver operating characteristic curve (AUROC) analysis.
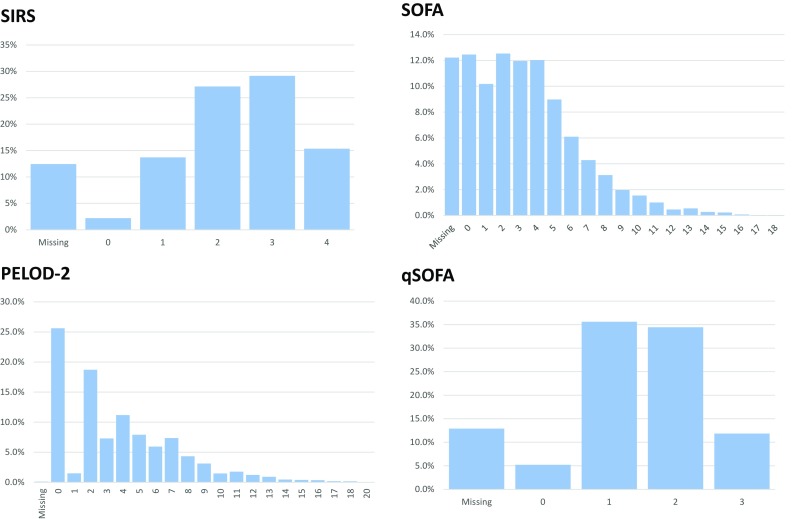
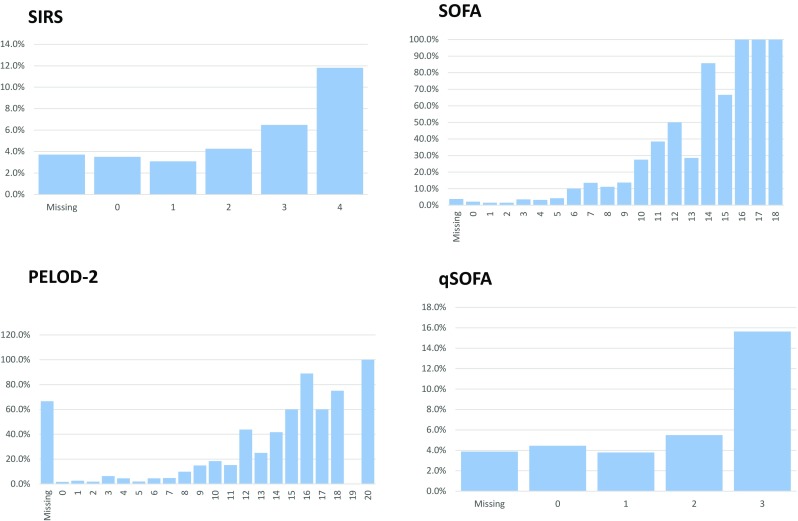
Results: Of 2594 paediatric ICU admissions due to infection, 151 (5.8%) children died, and 949/2594 (36.6%) patients died or experienced an ICU length of stay ≥ 3 days. A ≥ 2-point increase in the individual score was associated with a crude mortality increase from 3.1 to 6.8% for SIRS, from 1.9 to 7.6% for age-adapted SOFA, from 1.7 to 7.3% for PELOD-2, and from 3.9 to 8.1% for qSOFA (p < 0.001). The discrimination of outcomes was significantly higher for SOFA (adjusted AUROC 0.829; 0.791-0.868) and PELOD-2 (0.816; 0.777-0.854) than for qSOFA (0.739; 0.695-0.784) and SIRS (0.710; 0.664-0.756).
Conclusions: SIRS criteria lack specificity to identify children with infection at substantially higher risk of mortality. We demonstrate that adapting Sepsis-3 to age-specific criteria performs better than Sepsis-2-based criteria. Our findings support the translation of Sepsis-3 into paediatric-specific sepsis definitions and highlight the importance of robust paediatric organ dysfunction characterization.
Keywords: Childhood; Critical care; Infection; Mortality; PELOD; SIRS; SOFA; Scores; Sepsis.
Conflict of interest statement
None of the authors have declared a conflict of interest.
Figures
Comment in
-
Are septic children really just "septic little adults"?Intensive Care Med. 2018 Mar;44(3):392-394. doi: 10.1007/s00134-017-5041-4. Epub 2018 Jan 22. Intensive Care Med. 2018. PMID: 29356850 Free PMC article. No abstract available.
-
Which organ dysfunction scores to use in children with infection?Intensive Care Med. 2018 May;44(5):697-698. doi: 10.1007/s00134-018-5123-y. Epub 2018 Mar 22. Intensive Care Med. 2018. PMID: 29569156 No abstract available.
-
Paediatric sequential organ failure assessment score (pSOFA): a plea for the world-wide collaboration for consensus.Intensive Care Med. 2018 Jun;44(6):995-997. doi: 10.1007/s00134-018-5188-7. Epub 2018 Apr 27. Intensive Care Med. 2018. PMID: 29704146 No abstract available.
References
-
- Weiss SL, Fitzgerald JC, Pappachan J, Wheeler D, Jaramillo-Bustamante JC, Salloo A, Singhi SC, Erickson S, Roy JA, Bush JL, Nadkarni VM, Thomas NJ, Sepsis Prevalence O. Therapies Study I. Pediatric Acute Lung I. Sepsis Investigators N Global epidemiology of pediatric severe sepsis: the sepsis prevalence, outcomes, and therapies study. Am J Respir Crit Care Med. 2015;191:1147–1157. doi: 10.1164/rccm.201412-2323OC. - DOI - PMC - PubMed
-
- Schlapbach LJ, Straney L, Alexander J, MacLaren G, Festa M, Schibler A, Slater A, Group APS Mortality related to invasive infections, sepsis, and septic shock in critically ill children in Australia and New Zealand, 2002–13: a multicentre retrospective cohort study. Lancet Infect Dis. 2015;15:46–54. doi: 10.1016/S1473-3099(14)71003-5. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
