

A Case of Osteonecrosis of the Jaw in a Patient with Crohn's Disease Treated with Infliximab
- PMID: 29257800
- PMCID: PMC5737229
- DOI: 10.12659/AJCR.905355
A Case of Osteonecrosis of the Jaw in a Patient with Crohn's Disease Treated with Infliximab
Abstract
Patient: Female, 49
Final Diagnosis: Medication related osteonecrosis of the jaw
Symptoms: Painful bone exposure • pus discharge
Medication: Infliximab
Clinical Procedure: Surgical removal of necrotic bone
Specialty: Surgery
Objective:: Unusual clinical course
Background:: Medication-related osteonecrosis of the jaw (MRONJ) is a severe adverse drug reaction, occurring in patients undergoing treatments with antiresorptive or antiangiogenic agents, such as bisphosphonates, denosumab, or bevacizumab, for different oncologic and non-oncologic diseases. The aim of this study was to report a case of MRONJ in a patient taking infliximab, an anti-TNF-α antibody used to treat Crohn’s disease, rheumatoid arthritis, ulcerative colitis, ankylosing spondylitis, psoriatic arthritis, and plaque psoriasis.
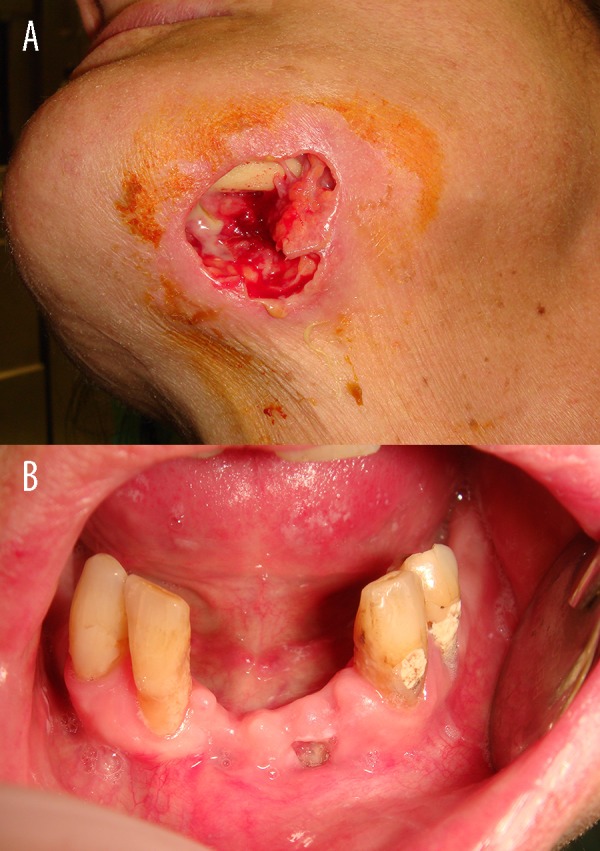
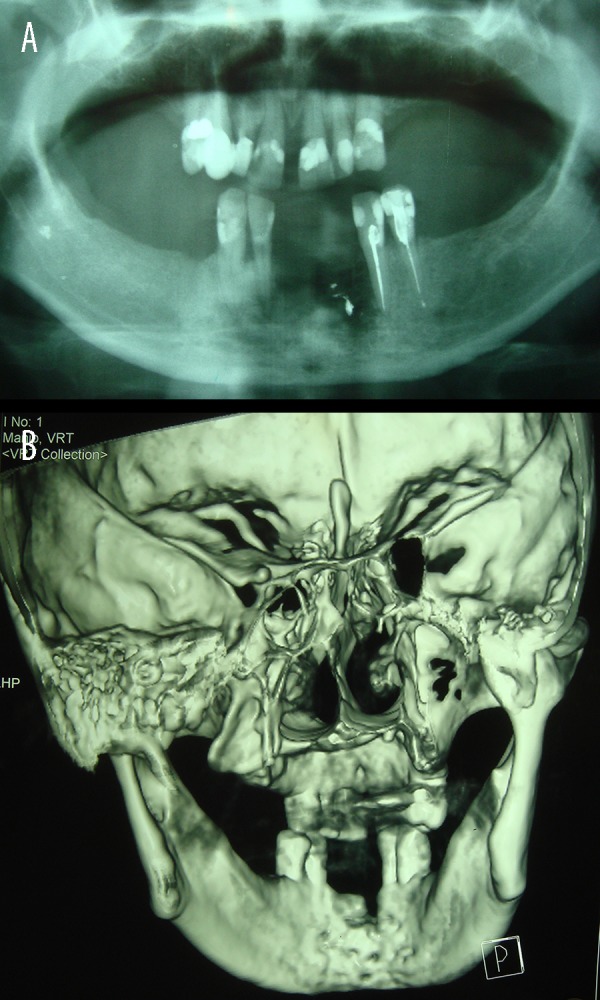
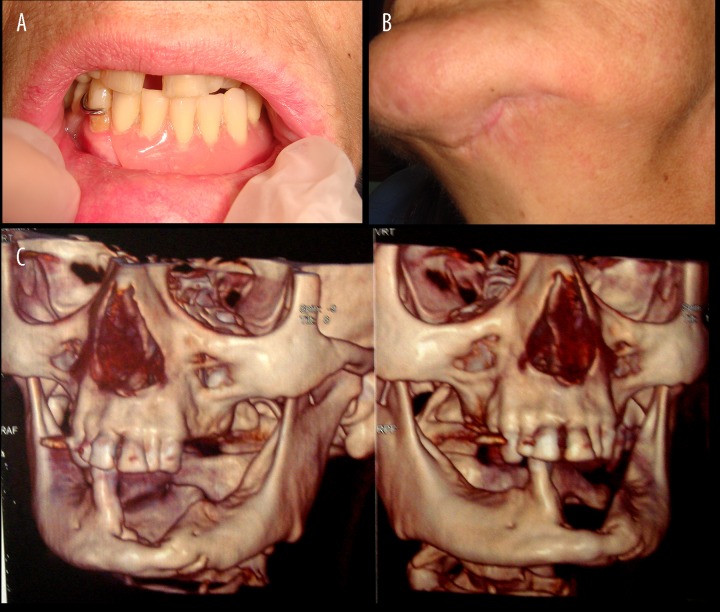
Case Report:: A 49-year-old female patient affected by Crohn’s disease, who had been undergoing 250 mg intravenous infliximab every six weeks for 12 years, with no history of antiresorptive or antiangiogenic agent administration, came to our attention for post-surgical MRONJ, associated with a wide cutaneous necrotic area of her anterior mandible. Following antibiotic cycles, the patient underwent surgical treatment with wide bone resection and debridement of necrotic tissues; after prolonged follow-up (16 months), the patient completely healed without signs of recurrence.
Conclusions:: Prevention of MRONJ by dental check-up before and during treatments with antiresorptive treatments (bisphosphonates or denosumab) is a well-established procedure. Although further studies are required to confirm the role of infliximab in MRONJ, based on the results of this study, we propose that patients who are going to be treated with infliximab should also undergo dental check-up before starting therapy, to possibly avoid MRONJ onset.
Keywords: Bisphosphonate-Associated Osteonecrosis of the Jaw; Bone Density Conservation Agents; Crohn Disease.
Conflict of interest statement
None.
Figures

References
-
- Ruggiero SL, Dodson TB, Fantasia J, et al. American Association of Oral and Maxillofacial Surgeons position paper on medication-related osteonecrosis of the jaws – 2014 update. J Oral Maxillofac Surg. 2014;72(10):1938–56. - PubMed
-
- Fleisher KE, Jolly A, Venkata UD, et al. Osteonecrosis of the jaw onset times are based on the route of bisphosphonate therapy. J Oral Maxillofac Surg. 2013;71:513–19. - PubMed
-
- Marx RE, Cillo JE, Jr, Ulloa JJ. Oral bisphosphonate-induced osteonecrosis: risk factors, prediction of risk using serum CTX testing, prevention, and treatment. J Oral Maxillofac Surg. 2007;65:2397–410. - PubMed
-
- Kos M, Kuebler JF, Luczak K, Engelke W. Bisphosphonate-related osteonecrosis of the jaws: A review of 34 cases and evaluation of risk. J Cranio-Maxillofac Surg. 2010;38:255–59. - PubMed
-
- Jadu F, Lee L, Pharoah M, Reece D, Wang L. A retrospective study assessing the incidence, risk factors and comorbidities of pamidronate-related necrosis of the jaws in multiple myeloma patients. Ann Oncol. 2007;18:2015–19. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
