

Significant value of 18F-FDG-PET/CT in diagnosing small cervical lymph node metastases in patients with nasopharyngeal carcinoma treated with intensity-modulated radiotherapy
- PMID: 29258597
- PMCID: PMC5738123
- DOI: 10.1186/s40880-017-0265-9
Significant value of 18F-FDG-PET/CT in diagnosing small cervical lymph node metastases in patients with nasopharyngeal carcinoma treated with intensity-modulated radiotherapy
Abstract
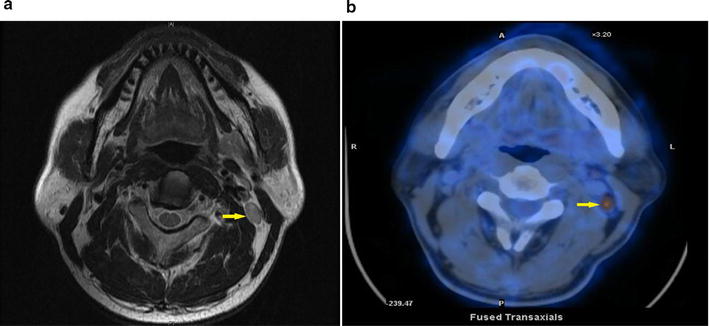
Background: Little is known about the nature of metastasis to small cervical lymph nodes (SCLNs) in the patients with nasopharyngeal carcinoma (NPC) examined by using 18-fluoro-2-deoxy-glucose (18F-FDG) positron emission tomography/computed tomography (PET/CT). The present study aimed to evaluate the diagnostic values of PET/CT in identifying metastasis in SCLNs in NPC patients.
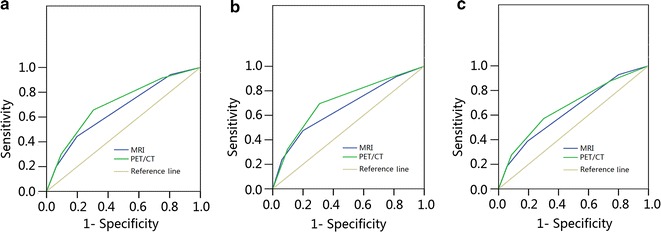
Methods: Magnetic resonance images (MRI) and PET/CT scans for 470 patients with newly diagnosed, non-distant metastatic NPC were analyzed. Metastatic rates of SCLNs were defined by the positive number of SCLNs on PET/CT scans and total number of SCLNs on MRI scans. Receiver operating characteristic curve was applied to compare PET/CT-determined stage with MRI-determined stage.
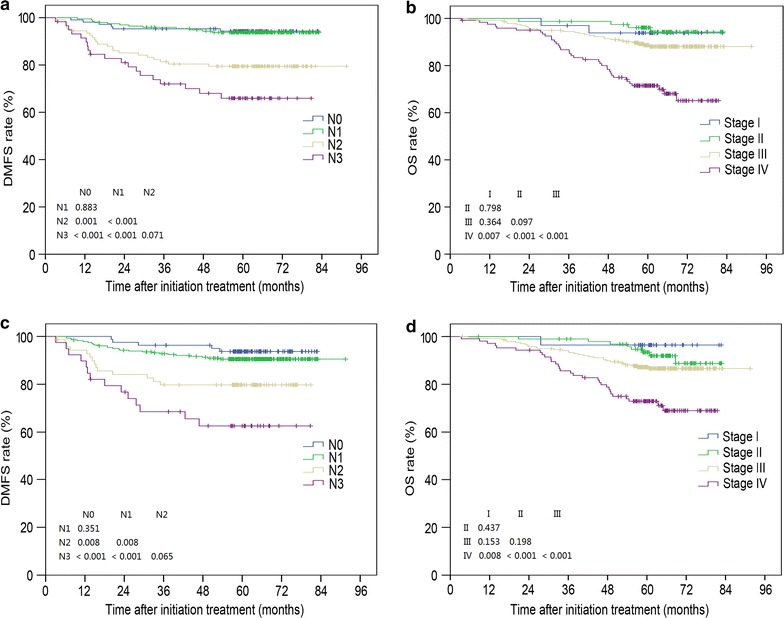
Results: In total, 2082 SCLNs were identified, with 808 (38.8%) ≥ 5 and < 6 mm in diameter (group A), 526 (25.3%) ≥ 6 and < 7 mm in diameter (group B), 374 (18.0%) ≥ 7 and < 8 mm in diameter (group C), 237 (11.4%) ≥ 8 and < 9 mm in diameter (group D), and 137 (6.5%) ≥ 9 and < 10 mm in diameter (group E). The overall metastatic rates examined by using PET/CT for groups A, B, C, D, and E were 3.5%, 8.0%, 31.3%, 60.0%, and 83.9%, respectively (P < 0.001). In level IV/Vb, the metastatic rate for nodes ≥ 8 mm was 84.6%. PET/CT examination resulted in modification of N category and overall stage for 135 (28.7%) and 46 (9.8%) patients, respectively. The areas under curve of MRI-determined and PET/CT-determined overall stage were 0.659 and 0.704 for predicting overall survival, 0.661 and 0.711 for predicting distant metastasis-free survival, and 0.636 and 0.663 for predicting disease-free survival.
Conclusions: PET/CT was more effective than MRI in identifying metastatic SCLNs, and the radiologic diagnostic criteria for metastatic lymph nodes in level IV/Vb should be re-defined.
Keywords: 18-fluoro-2-deoxy-glucose positron emission tomography with computed tomography (18F-PET/CT); Intensity-modulated radiotherapy; Magnetic resonance image; Nasopharyngeal carcinoma; Small cervical lymph nodes.
Figures
Similar articles
-
[Role of 18F-FDG PET/CT in diagnosis and staging of nasopharyngeal carcinoma].Ai Zheng. 2008 Sep;27(9):974-8. Ai Zheng. 2008. PMID: 18799039 Chinese.
-
[Evaluation of CT, MRI and PET-CT in detecting retropharyngeal lymph node metastasis in nasopharyngeal carcinoma].Ai Zheng. 2006 May;25(5):521-5. Ai Zheng. 2006. PMID: 16687067 Chinese.
-
Is unenhanced 18F-FDG-PET/CT better than enhanced CT in the detection of retropharyngeal lymph node metastasis in nasopharyngeal carcinoma?Ear Nose Throat J. 2016 Apr-May;95(4-5):178-84. Ear Nose Throat J. 2016. PMID: 27140019
-
Diagnostic accuracy of SUVmax in predicting malignancy of supraclavicular lymph nodes from primary oesophageal cancer.Eur J Radiol. 2020 Apr;125:108860. doi: 10.1016/j.ejrad.2020.108860. Epub 2020 Feb 11. Eur J Radiol. 2020. PMID: 32065926 Review.
-
Meta-analysis of diagnostic value of 18F-FDG PET or PET/CT for detecting lymph node and distant metastases in patients with nasopharyngeal carcinoma.Br J Radiol. 2014 Dec;87(1044):20140296. doi: 10.1259/bjr.20140296. Epub 2014 Oct 28. Br J Radiol. 2014. PMID: 25348201 Free PMC article. Review.
Cited by
-
The Chinese Society of Clinical Oncology (CSCO) clinical guidelines for the diagnosis and treatment of nasopharyngeal carcinoma.Cancer Commun (Lond). 2021 Nov;41(11):1195-1227. doi: 10.1002/cac2.12218. Epub 2021 Oct 26. Cancer Commun (Lond). 2021. PMID: 34699681 Free PMC article.
-
The role of initial 18F-FDG PET/CT in the management of patients with suspected extramedullary plasmocytoma.Cancer Imaging. 2018 May 15;18(1):19. doi: 10.1186/s40644-018-0152-x. Cancer Imaging. 2018. PMID: 29764500 Free PMC article.
-
A novel serum protein biomarker for the late-stage diagnosis of nasopharyngeal carcinoma.BMC Cancer. 2025 Apr 1;25(1):585. doi: 10.1186/s12885-025-13958-8. BMC Cancer. 2025. PMID: 40170144 Free PMC article.
-
A head-to-head comparison of 68Ga-DOTA-FAPI-04 and 18F-FDG PET/MR in patients with nasopharyngeal carcinoma: a prospective study.Eur J Nucl Med Mol Imaging. 2021 Sep;48(10):3228-3237. doi: 10.1007/s00259-021-05255-w. Epub 2021 Feb 20. Eur J Nucl Med Mol Imaging. 2021. PMID: 33609152
-
Radiotherapy versus Surgery in Early-Stage HPV-Positive Oropharyngeal Cancer.Cancer Res Treat. 2022 Apr;54(2):406-416. doi: 10.4143/crt.2021.441. Epub 2021 Jun 23. Cancer Res Treat. 2022. PMID: 34176249 Free PMC article.
References
-
- Baujat B, Audry H, Bourhis J, Chan AT, Onat H, Chua DT, et al. Chemotherapy in locally advanced nasopharyngeal carcinoma: an individual patient data meta-analysis of eight randomized trials and 1753 patients. Int J Radiat Oncol Biol Phys. 2006;64(1):47–56. doi: 10.1016/j.ijrobp.2005.06.037. - DOI - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
