

Hughes Abdominal Repair Trial (HART)-abdominal wall closure techniques to reduce the incidence of incisional hernias: feasibility trial for a multicentre, pragmatic, randomised controlled trial
- PMID: 29259055
- PMCID: PMC5778308
- DOI: 10.1136/bmjopen-2017-017235
Hughes Abdominal Repair Trial (HART)-abdominal wall closure techniques to reduce the incidence of incisional hernias: feasibility trial for a multicentre, pragmatic, randomised controlled trial
Abstract
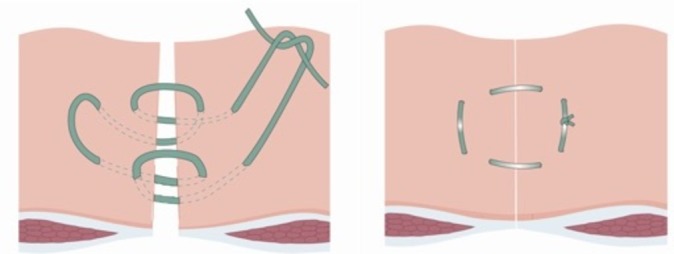
Objectives: Incisional hernias are common complications of midline abdominal closure. The 'Hughes Repair' combines a standard mass closure with a series of horizontal and two vertical mattress sutures within a single suture. There is evidence to suggest this technique is as effective as mesh repair for the operative management of incisional hernias; however, no trials have compared Hughes repair with standard mass closure for the prevention of incisional hernia formation. This paper aims to test the feasibility of running a randomised controlled trial of a comparison of abdominal wall closure methods following midline incisional surgery for colorectal cancer, in preparation to a definitive randomised controlled trial.
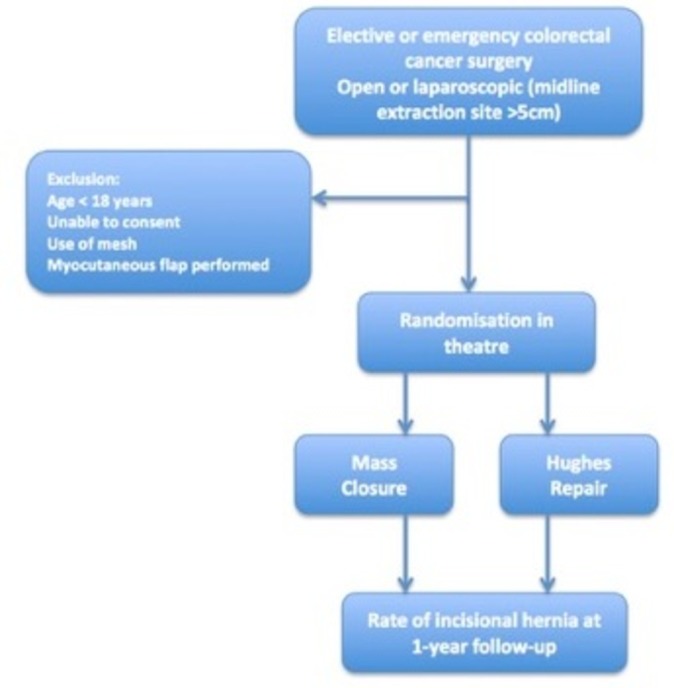
Design and setting: A feasibility trial (with 1:1 randomisation) conducted perioperatively during colorectal cancer surgery.
Participants: Patients undergoing midline incisional surgery for resection of colorectal cancer.
Interventions: Comparison of two suture techniques (Hughes repair or standard mass closure) for the closure of the midline abdominal wound following surgery for colorectal cancer.
Primary and secondary outcomes: A 30-patient feasibility trial assessed recruitment, randomisation, deliverability and early safety of the surgical techniques used.
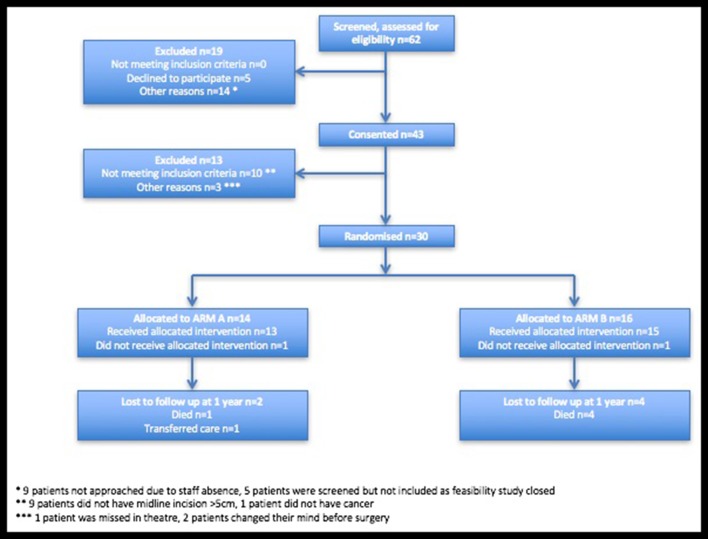
Results: A total of 30 patients were randomised from 43 patients recruited and consented, over a 5-month period. 14 and 16 patients were randomised to arms A and B, respectively. There was one superficial surgical site infection (SSI) and two organ space SSIs reported in arm A, and two superficial SSIs and one complete wound dehiscence in arm B. There were no suspected unexpected serious adverse reactions reported in either arm. Independent data monitoring committee found no early safety concerns.
Conclusions: The feasibility trial found no early safety concerns and demonstrated that the trial was acceptable to patients. Progression to the pilot and main phases of the trial has now commenced following approval by the independent data monitoring committee.
Trial registration number: ISRCTN 25616490.
Keywords: abdominal closure; colorectal cancer; hughes repair; incisional hernia; mass closure; randomised controlled trial.
© Article author(s) (or their employer(s) unless otherwise stated in the text of the article) 2017. All rights reserved. No commercial use is permitted unless otherwise expressly granted.
Conflict of interest statement
Competing interests: None declared.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical