

Mutational patterns in chemotherapy resistant muscle-invasive bladder cancer
- PMID: 29259186
- PMCID: PMC5736752
- DOI: 10.1038/s41467-017-02320-7
Mutational patterns in chemotherapy resistant muscle-invasive bladder cancer
Abstract
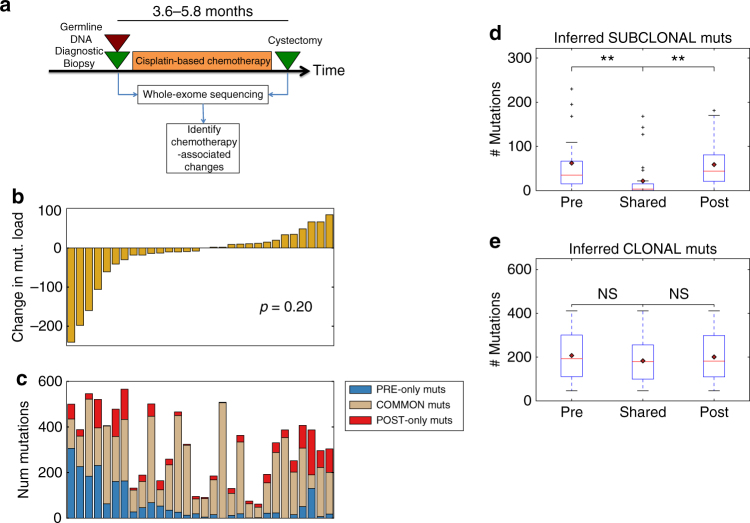
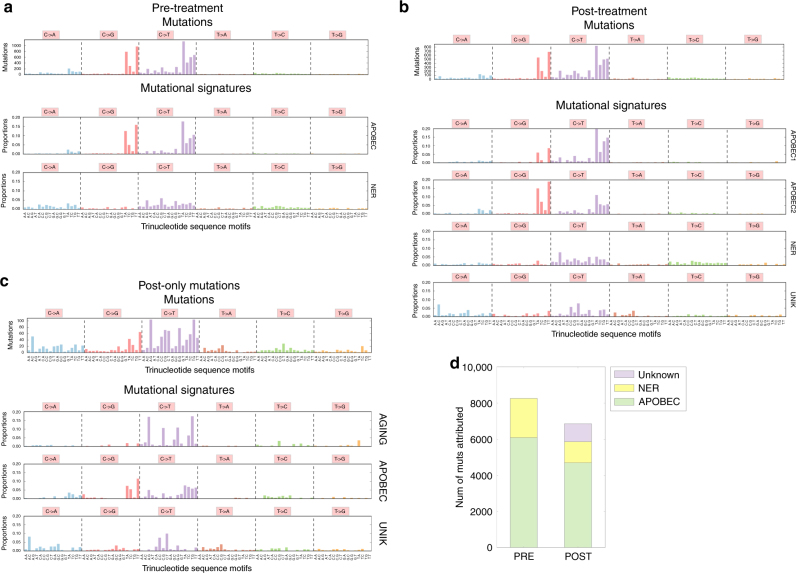
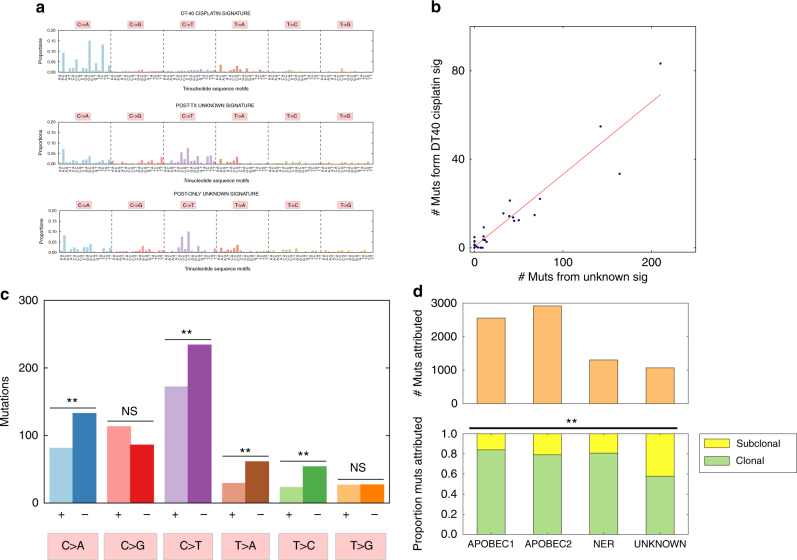
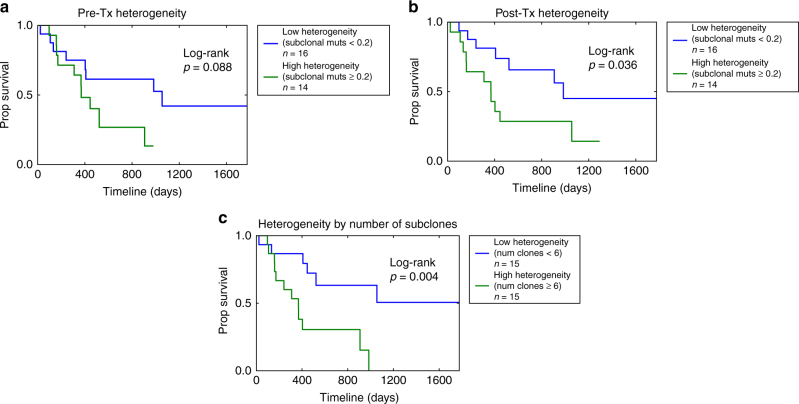
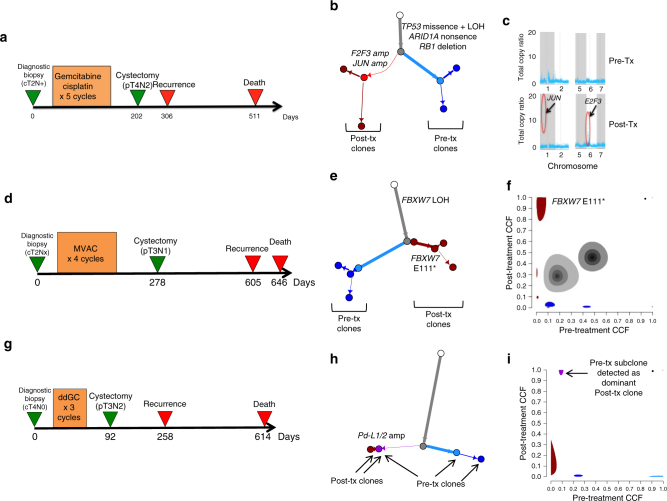
Despite continued widespread use, the genomic effects of cisplatin-based chemotherapy and implications for subsequent treatment are incompletely characterized. Here, we analyze whole exome sequencing of matched pre- and post-neoadjuvant cisplatin-based chemotherapy primary bladder tumor samples from 30 muscle-invasive bladder cancer patients. We observe no overall increase in tumor mutational burden post-chemotherapy, though a significant proportion of subclonal mutations are unique to the matched pre- or post-treatment tumor, suggesting chemotherapy-induced and/or spatial heterogeneity. We subsequently identify and validate a novel mutational signature in post-treatment tumors consistent with known characteristics of cisplatin damage and repair. We find that post-treatment tumor heterogeneity predicts worse overall survival, and further observe alterations in cell-cycle and immune checkpoint regulation genes in post-treatment tumors. These results provide insight into the clinical and genomic dynamics of tumor evolution with cisplatin-based chemotherapy, suggest mechanisms of clinical resistance, and inform development of clinically relevant biomarkers and trials of combination therapies.
Conflict of interest statement
The authors declare no competing financial interests.
Figures
Comment in
-
Re: Mutational Patterns in Chemotherapy Resistant Muscle-Invasive Bladder Cancer.J Urol. 2019 Jul;202(1):30-31. doi: 10.1097/01.JU.0000557727.39723.cd. Epub 2019 Jun 7. J Urol. 2019. PMID: 30925088 No abstract available.
References
-
- Reed, E. in Cancer Chemotherapy and Biotherapy: Principles and Practice 5th edn (eds Chabner B. & Longo D.) (Wolters Kluwer, 2010).
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
