

Diagnostic accuracy of high-resolution MRI as a method to predict potentially safe endoscopic and surgical planes in patients with early rectal cancer
- PMID: 29259791
- PMCID: PMC5730880
- DOI: 10.1136/bmjgast-2017-000151
Diagnostic accuracy of high-resolution MRI as a method to predict potentially safe endoscopic and surgical planes in patients with early rectal cancer
Abstract
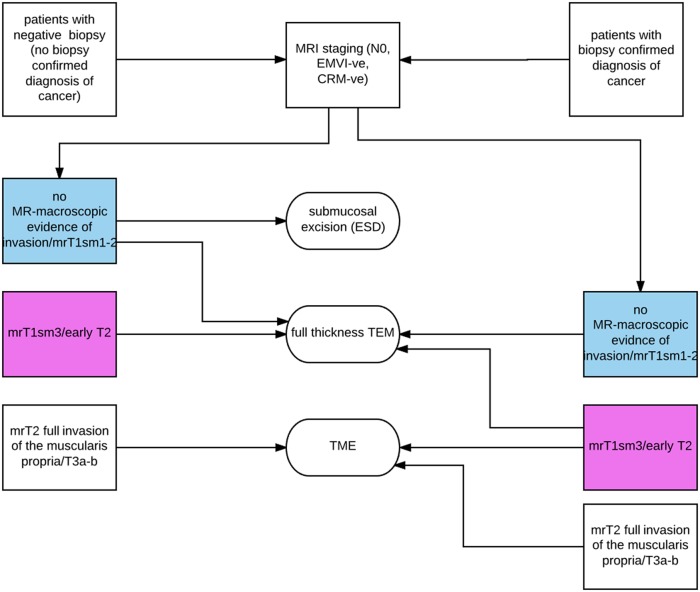
Introduction: Early rectal cancer (ERC) assessment should include prediction of the potential excision plane to safely remove lesions with clear deep margins and feasibility of organ preservation.
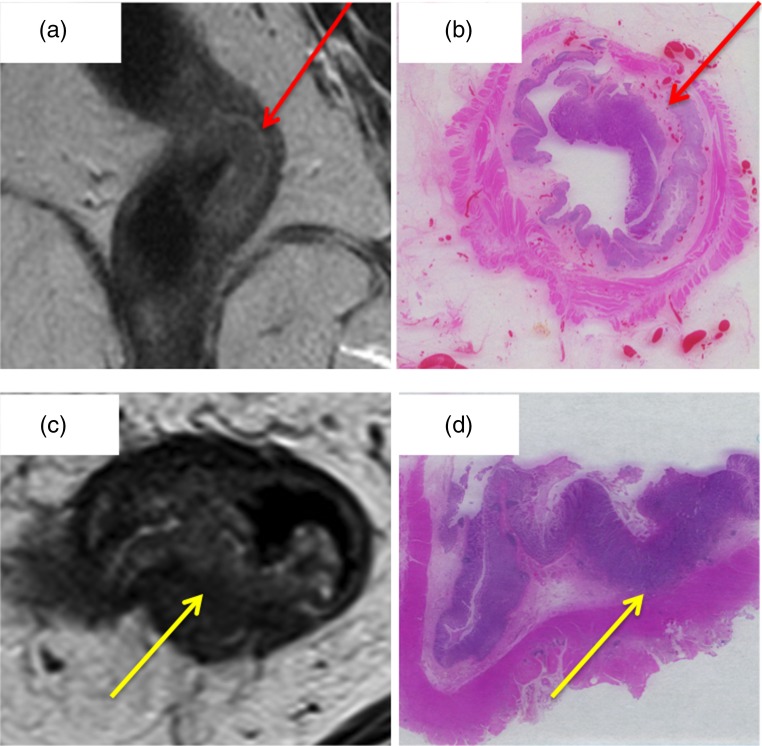
Method: MRI accuracy for differentiating ≤T1sm2 (partially preserved submucosa) or ≤T2 (partially preserved muscularis) versus >T2 tumours was compared with the gold standard of pT stage T1sm1/2 versus ≤pT2 versus >pT2. N stage was also compared. The MRI protocol employed a standard surface phased array coil with a high resolution (0.6×0.6×3 mm resolution). The staging data were analysed from a prospectively recorded database of all ERC (≤mrT3b) treated by primary surgery.
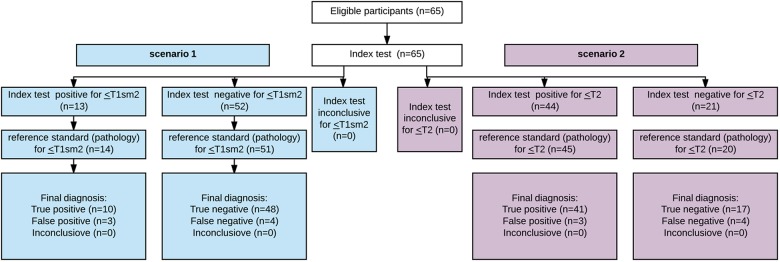
Results: Of 65 <mrT3b tumours, 45 were ≤pT2 and 14 were ≤pT1sm2. MRI accuracy for ≤T1sm2 was 89% (95% CI 63% to 87%), positive predictive value (PPV) 77% and negative predictive value (NPV) 92%, and for ≤T2 89% (95% CI 79% to 95%), PPV 93% and NPV 81%. Interobserver agreement between two experienced radiologists was >0.7 suggesting good agreement. 44 out of 65 patients underwent radical surgery and 22 out of 44 were ≤mrT2. MRI accuracy to predict lymph node status was 84% (95% CI 70% to 92%), PPV 71% and NPV 90%. Among the 21 out of 65 (32%) patients undergoing local excision or TEM, 20 out of 21 were staged as MR≤T2 and confirmed as such by pathology. On follow-up, none had relapse. If the decision had been made to offer local excision on MRI TN staging rather than clinical assessment, a significant increase in organ preservation surgery from 32% to 60% would have been observed (difference 23%, 95% CI 9% to 35%).
Conclusions: MRI is a useful tool for multidisciplinary teams (MDTs) wishing to optimise treatment options for ERC; these study findings will be validated in a prospective multicentre trial.
Keywords: ABDOMINAL MRI; COLORECTAL CANCER; ENDOSCOPIC POLYPECTOMY; STAGING.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- Muto T, Bussey HJ, Morson BC. The evolution of cancer of the colon and rectum. Cancer 1975;36:2251–70. doi:10.1002/cncr.2820360944 - DOI - PubMed
-
- Greenaway KJH, Khatun S, Kuryba A, et al. . National Bowel Cancer Audit Report 2015.
-
- Ashraf S, Hompes R, Slater A, et al. . A critical appraisal of endorectal ultrasound and transanal endoscopic microsurgery and decision-making in early rectal cancer. Colorectal Dis 2012;14:821–6. doi:10.1111/j.1463-1318.2011.02830.x - DOI - PubMed
-
- Williams JG, Pullan RD, Hill J, et al. . Management of the malignant colorectal polyp: ACPGBI position statement. Colorectal Dis 2013;15(Suppl 2):1–38. doi:10.1111/codi.12262 - DOI - PubMed
-
- Videhult P, Smedh K, Lundin P, et al. . Magnetic resonance imaging for preoperative staging of rectal cancer in clinical practice: high accuracy in predicting circumferential margin with clinical benefit. Colorectal Dis 2007;9:412–19. doi:10.1111/j.1463-1318.2006.01167.x - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical