

CD4 count and tuberculosis risk in HIV-positive adults not on ART: a systematic review and meta-analysis
- PMID: 29259846
- PMCID: PMC5733368
- DOI: 10.7717/peerj.4165
CD4 count and tuberculosis risk in HIV-positive adults not on ART: a systematic review and meta-analysis
Abstract
Background: CD4 cell count in adults with human immunodeficiency virus (HIV) infection (PLHIV) not receiving antiretroviral therapy (ART) influences tuberculosis (TB) risk. Despite widespread use in models informing resource allocation, this relationship has not been systematically reviewed.
Methods: We systematically searched MEDLINE, Aidsinfo, Cochrane review database and Google Scholar for reports in English describing TB incidence stratified by updated CD4 cell count in cohorts of HIV-positive adults (age ≥15 years) not on ART (PROSPERO protocol no: CRD42016048888). Among inclusion criteria were: reporting precision for TB incidence, repeated CD4 measurements, and TB incidence reported for those not on ART or monotherapy. Study quality was assessed via the Newcastle-Ottawa tool for cohort studies. A Bayesian hierarchical model was fitted to estimate the pooled factor increase in TB incidence with respect to CD4 cell count decrement.
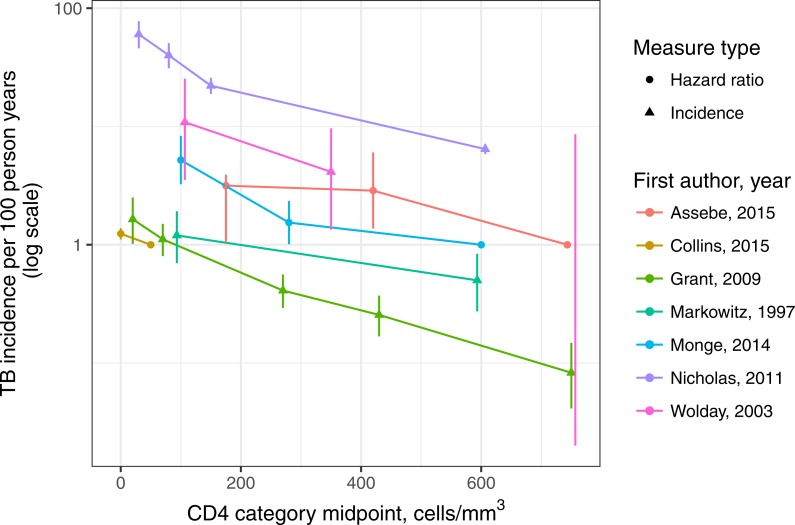
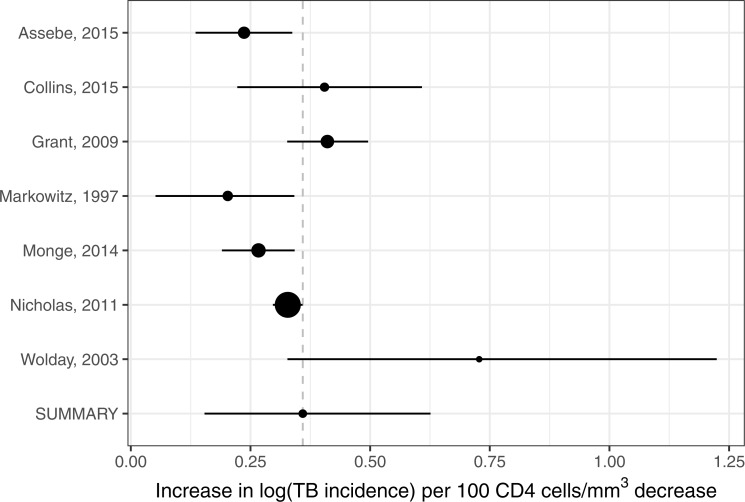
Results: A total of 1,555 distinct records were identified from which 164 full text articles were obtained. Common reasons for exclusion of full texts were: no valid TB incidence, no repeat CD4 measurements, and not reporting TB incidence by ART status. The seven studies included reported on 1,206 TB cases among 41,271 individuals, with a typical median follow-up of four years. Studies were generally rated as moderate or high quality. Our meta-analysis estimated a 1.43 (95% credible interval: 1.16-1.88)-fold increase in TB incidence per 100 cells per mm3 decrease in CD4 cell count.
Discussion: Our analysis confirms previous estimates of exponential increase in TB incidence with declining CD4 cell count in adults, emphasizing the importance of early ART initiation to reduce TB risk in PLHIV.
Keywords: Antiretroviral therapy; CD4 cell count; Modeling; Opportunistic infections; TB.
Conflict of interest statement
The authors declare there are no competing interests.
Figures


References
-
- Assebe LF, Reda HL, Wubeneh AD, Lerebo WT, Lambert SM. The effect of isoniazid preventive therapy on incidence of tuberculosis among HIV-infected clients under pre-ART care, Jimma, Ethiopia: a retrospective cohort study. BMC Public Health. 2015;15:346. doi: 10.1186/s12889-015-1719-0. - DOI - PMC - PubMed
-
- Ayubi E, Doosti-Irani A, Sanjari Moghaddam A, Sani M, Nazarzadeh M, Mostafavi E. The clinical usefulness of tuberculin skin test versus interferon-gamma release assays for diagnosis of latent tuberculosis in HIV patients: a meta-analysis. PLOS ONE. 2016;11:e0161983. doi: 10.1371/journal.pone.0161983. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
