

Reversal of carotid dissection-induced ocular and cerebral ischemia by stenting
- PMID: 29260078
- PMCID: PMC5722172
- DOI: 10.1016/j.ajoc.2017.05.003
Reversal of carotid dissection-induced ocular and cerebral ischemia by stenting
Abstract
Purpose: To present an example of how close clinical monitoring of a patient with acute Horner syndrome from carotid artery dissection may be critical in reversing neurologic dysfunction.
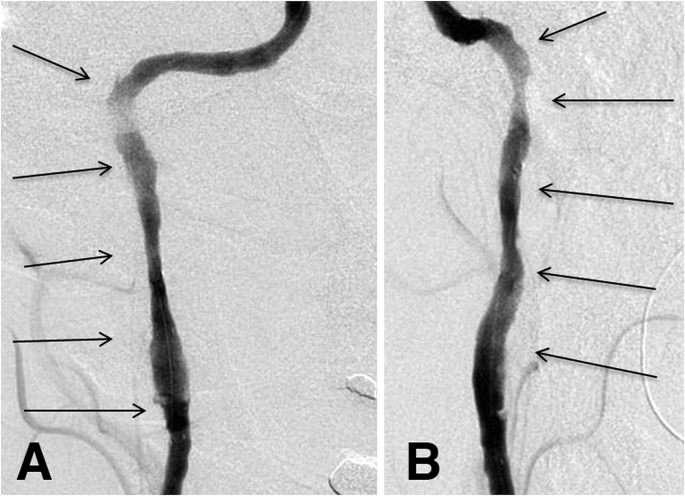
Observations: A patient whose initial neuro-ophthalmic manifestation was Horner syndrome, but who evolved over 14 days to display transient monocular vision loss, ipsilateral ocular ischemic syndrome, and episodic contralateral hemiparesis. Digital subtraction angiography demonstrated progressive ipsilateral carotid occlusion with lack of collateral flow. The patient underwent stenting with rapid reversal of transient monocular visual loss and hemiparesis. Follow-up examination several months later confirmed complete resolution of all clinical abnormalities.
Conclusions and importance: This case displayed protracted evolution of ischemic manifestations following carotid artery dissection and their prompt reversal with stenting. This case emphasizes the value of close clinical attention to a patient with acute Horner syndrome because manifestations may appear more than 10 days after event onset that impel intervention for the dissection.
Keywords: Carotid artery dissection; Carotid artery stenting; Hemiparesis; Horner syndrome; Ischemic ocular syndrome.
Figures



Similar articles
-
Internal Carotid Artery Dissection Presenting with Transient or Subclinical Horner Syndrome.Case Rep Ophthalmol. 2024 Jan 9;15(1):29-35. doi: 10.1159/000535475. eCollection 2024 Jan-Dec. Case Rep Ophthalmol. 2024. PMID: 38196925 Free PMC article.
-
Percutaneous carotid artery angioplasty and stenting for ocular ischemic syndrome.Ophthalmology. 2004 Dec;111(12):2284-91. doi: 10.1016/j.ophtha.2004.05.029. Ophthalmology. 2004. PMID: 15582088
-
Blindness Following Carotid Artery Stenting Due to Ocular Hyperperfusion - Report and Review of Literature.Neurol India. 2020 Jul-Aug;68(4):897-899. doi: 10.4103/0028-3886.293455. Neurol India. 2020. PMID: 32859837 Review.
-
A Case of Complete Recovery of Fluctuating Monocular Blindness Following Endovascular Treatment in Internal Carotid Artery Dissection.J Stroke Cerebrovasc Dis. 2015 Sep;24(9):e283-6. doi: 10.1016/j.jstrokecerebrovasdis.2015.06.029. Epub 2015 Jul 17. J Stroke Cerebrovasc Dis. 2015. PMID: 26194847
-
Vascular emergencies in neuro-ophthalmology.Rom J Ophthalmol. 2020 Oct-Dec;64(4):323-332. doi: 10.22336/rjo.2020.54. Rom J Ophthalmol. 2020. PMID: 33367170 Free PMC article. Review.
Cited by
-
Amalric choroidal infarction, retinal artery occlusion, and ischemic optic neuropathy: Delayed presentations of traumatic internal carotid artery dissection.Am J Ophthalmol Case Rep. 2024 Oct 11;36:102193. doi: 10.1016/j.ajoc.2024.102193. eCollection 2024 Dec. Am J Ophthalmol Case Rep. 2024. PMID: 39498145 Free PMC article.
-
Ocular ischemic syndrome secondary to cerebral aneurysms.Am J Ophthalmol Case Rep. 2024 Oct 31;36:102214. doi: 10.1016/j.ajoc.2024.102214. eCollection 2024 Dec. Am J Ophthalmol Case Rep. 2024. PMID: 39553911 Free PMC article.
References
-
- Patel R.R., Adam R., Maldjian C., Lincoln C.M., Yuen A., Arneja A. Cervical carotid artery dissection: current review of diagnosis and treatment. Cardiol Rev. 2012;20:145–152. - PubMed
-
- Biousse V., Touboul P.J., D'Anglejan-Chatillon J., Lévy C., Schaison M., Bousser M.G. Ophthalmologic manifestations of internal carotid artery dissection. Am J Ophthalmol. 1998;126:565–577. - PubMed
-
- Mendrinos E., Machinis T.G., Pournaras C.J. Ocular ischemic syndrome. Surv Ophthalmol. 2010;55:2–34. - PubMed
-
- Duker J.S., Belmont J.B. Ocular ischemic syndrome secondary to carotid artery dissection. Am J Ophthalmol. 1988;106:750–752. - PubMed
-
- Lee V.H., Brown R.D., Jr., Mandrekar J.N., Mokri B. Incidence and outcome of cervical artery dissection: a population-based study. Neurology. 2006;67:1809. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
