

Association of Broad- vs Narrow-Spectrum Antibiotics With Treatment Failure, Adverse Events, and Quality of Life in Children With Acute Respiratory Tract Infections
- PMID: 29260224
- PMCID: PMC5820700
- DOI: 10.1001/jama.2017.18715
Association of Broad- vs Narrow-Spectrum Antibiotics With Treatment Failure, Adverse Events, and Quality of Life in Children With Acute Respiratory Tract Infections
Abstract
Importance: Acute respiratory tract infections account for the majority of antibiotic exposure in children, and broad-spectrum antibiotic prescribing for acute respiratory tract infections is increasing. It is not clear whether broad-spectrum treatment is associated with improved outcomes compared with narrow-spectrum treatment.
Objective: To compare the effectiveness of broad-spectrum and narrow-spectrum antibiotic treatment for acute respiratory tract infections in children.
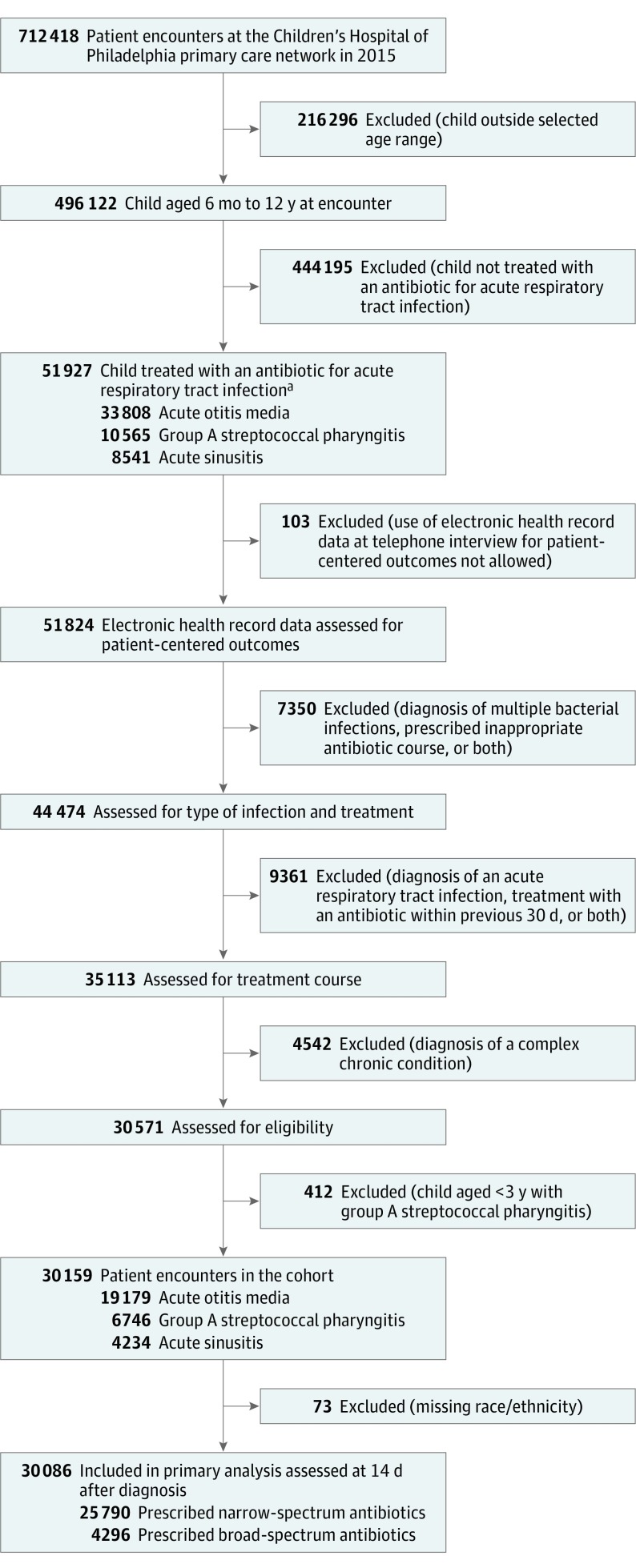
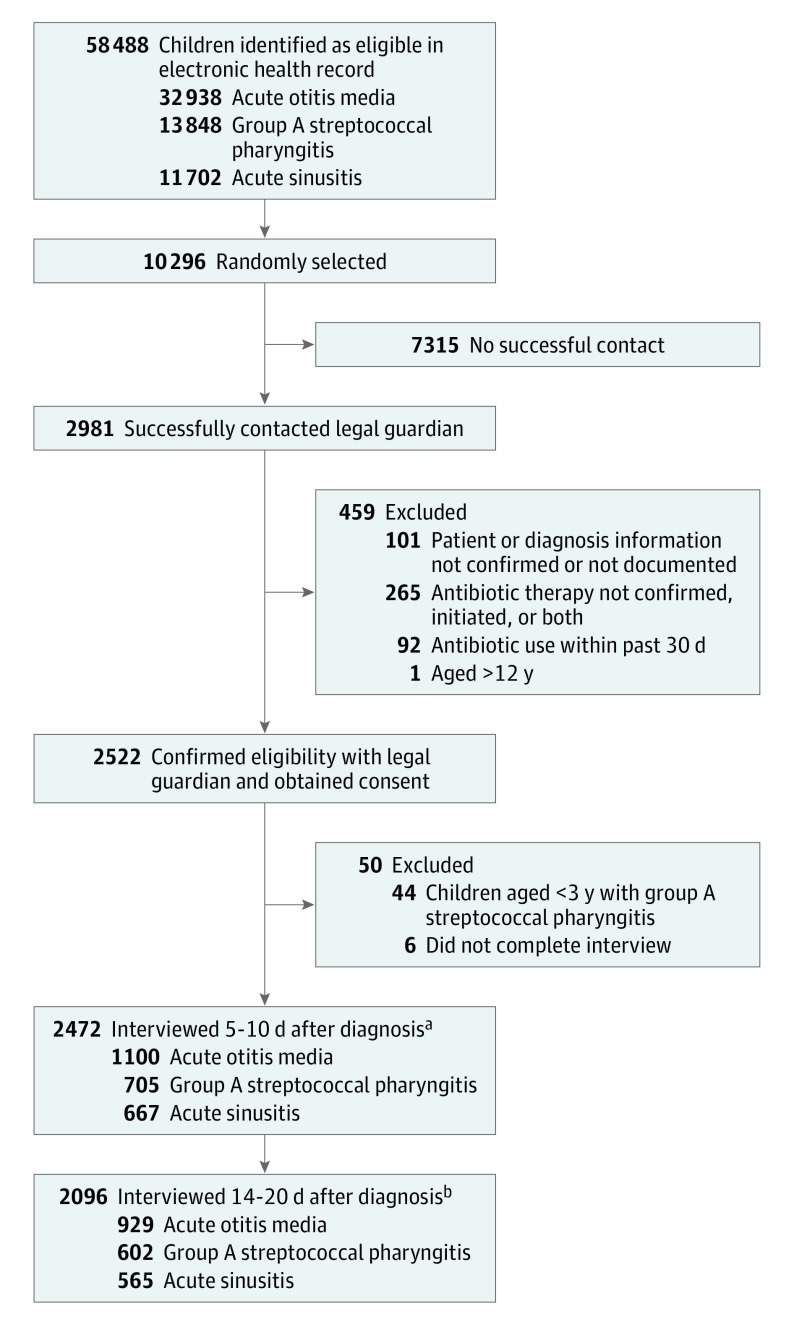
Design, setting, and participants: A retrospective cohort study assessing clinical outcomes and a prospective cohort study assessing patient-centered outcomes of children between the ages of 6 months and 12 years diagnosed with an acute respiratory tract infection and prescribed an oral antibiotic between January 2015 and April 2016 in a network of 31 pediatric primary care practices in Pennsylvania and New Jersey. Stratified and propensity score-matched analyses to account for confounding by clinician and by patient-level characteristics, respectively, were implemented for both cohorts.
Exposures: Broad-spectrum antibiotics vs narrow-spectrum antibiotics.
Main outcomes and measures: In the retrospective cohort, the primary outcomes were treatment failure and adverse events 14 days after diagnosis. In the prospective cohort, the primary outcomes were quality of life, other patient-centered outcomes, and patient-reported adverse events.
Results: Of 30 159 children in the retrospective cohort (19 179 with acute otitis media; 6746, group A streptococcal pharyngitis; and 4234, acute sinusitis), 4307 (14%) were prescribed broad-spectrum antibiotics including amoxicillin-clavulanate, cephalosporins, and macrolides. Broad-spectrum treatment was not associated with a lower rate of treatment failure (3.4% for broad-spectrum antibiotics vs 3.1% for narrow-spectrum antibiotics; risk difference for full matched analysis, 0.3% [95% CI, -0.4% to 0.9%]). Of 2472 children enrolled in the prospective cohort (1100 with acute otitis media; 705, group A streptococcal pharyngitis; and 667, acute sinusitis), 868 (35%) were prescribed broad-spectrum antibiotics. Broad-spectrum antibiotics were associated with a slightly worse child quality of life (score of 90.2 for broad-spectrum antibiotics vs 91.5 for narrow-spectrum antibiotics; score difference for full matched analysis, -1.4% [95% CI, -2.4% to -0.4%]) but not with other patient-centered outcomes. Broad-spectrum treatment was associated with a higher risk of adverse events documented by the clinician (3.7% for broad-spectrum antibiotics vs 2.7% for narrow-spectrum antibiotics; risk difference for full matched analysis, 1.1% [95% CI, 0.4% to 1.8%]) and reported by the patient (35.6% for broad-spectrum antibiotics vs 25.1% for narrow-spectrum antibiotics; risk difference for full matched analysis, 12.2% [95% CI, 7.3% to 17.2%]).
Conclusions and relevance: Among children with acute respiratory tract infections, broad-spectrum antibiotics were not associated with better clinical or patient-centered outcomes compared with narrow-spectrum antibiotics, and were associated with higher rates of adverse events. These data support the use of narrow-spectrum antibiotics for most children with acute respiratory tract infections.
Conflict of interest statement
Figures
Comment in
-
Narrow-spectrum, compared with broad-spectrum, antibiotics equally effective with less adverse events.J Pediatr. 2018 May;196:324-327. doi: 10.1016/j.jpeds.2018.02.054. J Pediatr. 2018. PMID: 29703366 No abstract available.
-
Broad-spectrum antibiotics gave no clinical benefit and more adverse effects than narrow-spectrum antibiotics in treating acute respiratory tract infections in US children.BMJ Evid Based Med. 2019 Jun;24(3):119-120. doi: 10.1136/bmjebm-2018-110938. Epub 2018 Oct 25. BMJ Evid Based Med. 2019. PMID: 30361328 No abstract available.
References
-
- Chai G, Governale L, McMahon AW, Trinidad JP, Staffa J, Murphy D. Trends of outpatient prescription drug utilization in US children, 2002-2010. Pediatrics. 2012;130(1):23-31. - PubMed
-
- Hersh AL, Shapiro DJ, Pavia AT, Shah SS. Antibiotic prescribing in ambulatory pediatrics in the United States. Pediatrics. 2011;128(6):1053-1061. - PubMed
-
- Steinman MA, Landefeld CS, Gonzales R. Predictors of broad-spectrum antibiotic prescribing for acute respiratory tract infections in adult primary care. JAMA. 2003;289(6):719-725. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
