

Lithium-Associated Hypercalcemia: Pathophysiology, Prevalence, Management
- PMID: 29260296
- PMCID: PMC5762804
- DOI: 10.1007/s00268-017-4328-5
Lithium-Associated Hypercalcemia: Pathophysiology, Prevalence, Management
Abstract
Background: Lithium-associated hypercalcemia (LAH) is an ill-defined endocrinopathy. The aim of the present study was to determine the prevalence of hypercalcemia in a cohort of bipolar patients (BP) with and without concomitant lithium treatment and to study surgical outcomes for lithium-associated hyperparathyroidism.
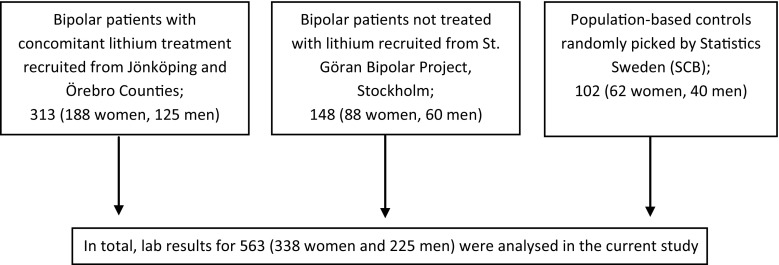
Methods: Retrospective data, including laboratory results, surgical outcomes and medications, were collected from 313 BP treated with lithium from two psychiatric outpatient units in central Sweden. In addition, data were collected from 148 BP without lithium and a randomly selected control population of 102 individuals. Logistic regression was used to compare odds of hypercalcemia in these respective populations.
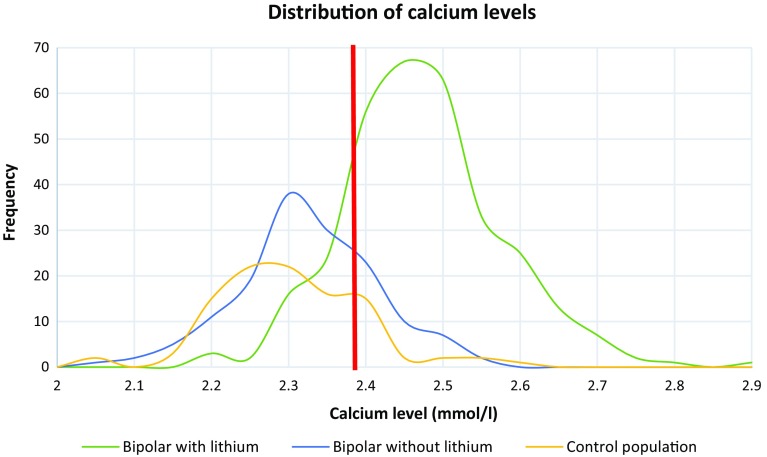
Results: The prevalence of lithium-associated hypercalcemia was 26%. Mild hypercalcemia was detected in 87 out of 563 study participants. The odds of hypercalcemia were significantly higher in BP with lithium treatment compared with BP unexposed to lithium (adjusted OR 13.45; 95% CI 3.09, 58.55; p = 0.001). No significant difference was detected between BP without lithium and control population (adjusted OR 2.40; 95% CI 0.38, 15.41; p = 0.355). Seven BP with lithium underwent surgery where an average of two parathyroid glands was removed. Parathyroid hyperplasia was present in four patients (57%) at the initial operation. One patient had persistent disease after the initial operation, and six patients had recurrent disease at follow-up time which was on average 10 years.
Conclusion: The high prevalence of LAH justifies the regular monitoring of calcium homeostasis, particularly in high-risk groups. If surgery is necessary, bilateral neck exploration should be considered in patients on chronic lithium treatment. Prospective studies are needed.
Conflict of interest statement
All authors declare no conflict of interest.
Figures
References
-
- Cade JF. Lithium salts in the treatment of psychotic excitement. Med J Aust. 1949;2:349–352. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
