

Cell salvage and donor blood transfusion during cesarean section: A pragmatic, multicentre randomised controlled trial (SALVO)
- PMID: 29261655
- PMCID: PMC5736174
- DOI: 10.1371/journal.pmed.1002471
Cell salvage and donor blood transfusion during cesarean section: A pragmatic, multicentre randomised controlled trial (SALVO)
Abstract
Background: Excessive haemorrhage at cesarean section requires donor (allogeneic) blood transfusion. Cell salvage may reduce this requirement.
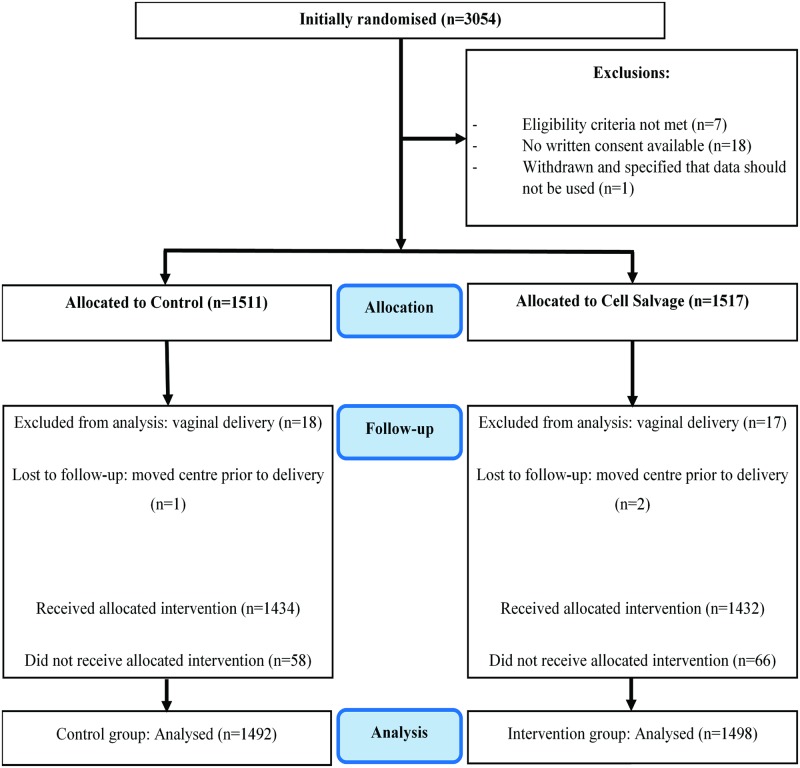
Methods and findings: We conducted a pragmatic randomised controlled trial (at 26 obstetric units; participants recruited from 4 June 2013 to 17 April 2016) of routine cell salvage use (intervention) versus current standard of care without routine salvage use (control) in cesarean section among women at risk of haemorrhage. Randomisation was stratified, using random permuted blocks of variable sizes. In an intention-to-treat analysis, we used multivariable models, adjusting for stratification variables and prognostic factors identified a priori, to compare rates of donor blood transfusion (primary outcome) and fetomaternal haemorrhage ≥2 ml in RhD-negative women with RhD-positive babies (a secondary outcome) between groups. Among 3,028 women randomised (2,990 analysed), 95.6% of 1,498 assigned to intervention had cell salvage deployed (50.8% had salvaged blood returned; mean 259.9 ml) versus 3.9% of 1,492 assigned to control. Donor blood transfusion rate was 3.5% in the control group versus 2.5% in the intervention group (adjusted odds ratio [OR] 0.65, 95% confidence interval [CI] 0.42 to 1.01, p = 0.056; adjusted risk difference -1.03, 95% CI -2.13 to 0.06). In a planned subgroup analysis, the transfusion rate was 4.6% in women assigned to control versus 3.0% in the intervention group among emergency cesareans (adjusted OR 0.58, 95% CI 0.34 to 0.99), whereas it was 2.2% versus 1.8% among elective cesareans (adjusted OR 0.83, 95% CI 0.38 to 1.83) (interaction p = 0.46). No case of amniotic fluid embolism was observed. The rate of fetomaternal haemorrhage was higher with the intervention (10.5% in the control group versus 25.6% in the intervention group, adjusted OR 5.63, 95% CI 1.43 to 22.14, p = 0.013). We are unable to comment on long-term antibody sensitisation effects.
Conclusions: The overall reduction observed in donor blood transfusion associated with the routine use of cell salvage during cesarean section was not statistically significant.
Trial registration: This trial was prospectively registered on ISRCTN as trial number 66118656 and can be viewed on http://www.isrctn.com/ISRCTN66118656.
Conflict of interest statement
I have read the journal’s policy and the authors of this manuscript have the following competing interests: Primary NIHR grant supporting the roles of KK, PM, RH, IW, LB, TR, CM, JDa, SR, DL and JDo. PM also declares having been a co-applicant for two other NIHR-funded grants over within the last five years. Other than this, all authors declare no support from any organisation for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
Figures
Comment in
-
Association of Anaesthetists guidelines on cell salvage - a backward step for obstetric practice?Anaesthesia. 2018 Dec;73(12):1574-1575. doi: 10.1111/anae.14464. Anaesthesia. 2018. PMID: 30412294 No abstract available.
References
-
- Betran AP, Torloni MR, Zhang JJ, Gülmezoglu AM, WHO Working Group on Caesarean Section. WHO statement on caesarean section rates. BJOG. 2016;123(5):667–70. doi: 10.1111/1471-0528.13526 - DOI - PMC - PubMed
-
- Centre for Maternal and Child Enquiries. Saving mothers lives: reviewing maternal deaths to make motherhood safer: 2006–2008. BJOG. 2011;118(Suppl 1):1–203. - PubMed
-
- Bodelon C, Bernabe-Ortiz A, Schiff MA, Reed SD. Factors associated with peripartum hysterectomy. Obstet Gynecol. 2009;114(1):115–23. doi: 10.1097/AOG.0b013e3181a81cdd - DOI - PMC - PubMed
-
- Intensive Care National Audit & Research Centre. Female admissions (aged 16–50 years) to adult, general critical care units in England, Wales and Northern Ireland reported as ‘currently pregnant’ or ‘recently pregnant’. London: Obstetric Anaesthetists’ Association; 2013.
-
- Bateman BT, Berman MF, Riley LE, Leffert LR. The epidemiology of postpartum hemorrhage in a large, nationwide sample of deliveries. Anesth Analg. 2010;110(5):1368–73. doi: 10.1213/ANE.0b013e3181d74898 - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
