

Aging and decreased glomerular filtration rate: An elderly population-based study
- PMID: 29261774
- PMCID: PMC5736213
- DOI: 10.1371/journal.pone.0189935
Aging and decreased glomerular filtration rate: An elderly population-based study
Abstract
Background: Although a reduced glomerular filtration rate (GFR) in old people has been attributed to physiologic aging, it may be associated with kidney disease or superimposed comorbidities. This study aims to assess the prevalence of decreased GFR in a geriatric population in a developing country and its prevalence in the absence of simultaneous diseases.
Study design and methods: This is a cross-sectional study of data from the Saúde, Bem-Estar e Envelhecimento cohort study (SABE study[Health, Well-Being and Aging]), a multiple cohorts study. A multistage cluster sample composed of 1,253 individuals representative of 1,249,388 inhabitants of São Paulo city aged ≥60 years in 2010 was analyzed. The participants answered a survey on socio-demographic factors and health, had blood pressure measured and urine and blood samples collected. GFR was estimated and defined as decreased when <60 mL/min/1.73m2. Kidney damage was defined as dipstick-positive hematuria or urinary protein:creatinine > 0.20 g/g.
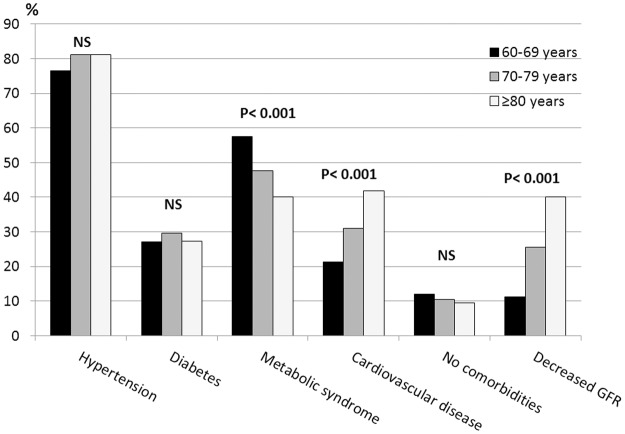
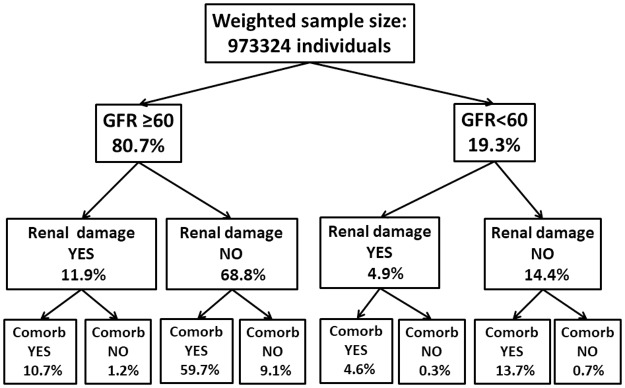
Results: The prevalence of GFR <60 mL/min/1.73m2 was 19.3%. Individuals with GFR <60 mL/min/1.73m2 were older (75±1 versus 69±1 years, p<0.001), had lower schooling (18 versus 30% with complete 8-year basic cycle, p = 0.010), and higher prevalence of hypertension (82 versus 63%, p<0.001), diabetes (34 versus 26%, p = 0.021), cardiovascular disease (43 versus 24%, p<0.001) and kidney damage (35% versus 15%, p<0.001). Only 0.7% of the entire studied population had GFR <60 mL/min/1.73m2 without simultaneous diseases or kidney damage. Among the individuals with GFR <60 mL/min/1.73m2, 3.5% had neither renal damage nor associated comorbidities, whereas among those with GFR ≥60 mL/min/1.73m2, 11.0% had none of these conditions. Logistic regression showed that older age, cardiovascular disease and hypertension were associated with GFR<60 mL/min/1.73m2.
Conclusions: Decreased GFR was highly prevalent among the geriatric population in a megalopolis of a developing country. It was rarely present without simultaneous chronic comorbidities or kidney damage.
Conflict of interest statement
Figures
References
-
- Zhang Q-L, Rothenbacher D. Prevalence of chronic kidney disease in population-based studies: Systematic review. BMC Public Health. 2008;8:117 doi: 10.1186/1471-2458-8-117 - DOI - PMC - PubMed
-
- United States Renal Data System. 2015 USRDS annual data report. Epidemiology of kidney disease in the United States. National Institutes of Health, National Institute of Diabetes and Kidney Diseases, Bethesda, MD, 2015. www.usrds.org/2015/view/default.aspx. Accessed July 6, 2016.
-
- de Lima AO, Kesrouani S, Gomes RA, Cruz J, Mastroianni-Kirsztajn G. Population screening for chronic kidney disease: a survey involving 38 721 Brazilians. Nephrol Dial Transplant. 2012;27(Suppl 3):iii135–138. doi: 10.1093/ndt/gfs063 - DOI - PubMed
-
- Sesso RCC, Lopes AA, Thomé FS, Watanabe Y, dos Santos DR. Report of the Brazilian Chronic Dialysis Census 2012. J Bras Nefrol. 2014;36:48–53. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
