

Endoscopic Treatment versus Shunting for Infant Hydrocephalus in Uganda
- PMID: 29262276
- PMCID: PMC5784827
- DOI: 10.1056/NEJMoa1707568
Endoscopic Treatment versus Shunting for Infant Hydrocephalus in Uganda
Abstract
Background: Postinfectious hydrocephalus in infants is a major health problem in sub-Saharan Africa. The conventional treatment is ventriculoperitoneal shunting, but surgeons are usually not immediately available to revise shunts when they fail. Endoscopic third ventriculostomy with choroid plexus cauterization (ETV-CPC) is an alternative treatment that is less subject to late failure but is also less likely than shunting to result in a reduction in ventricular size that might facilitate better brain growth and cognitive outcomes.
Methods: We conducted a randomized trial to evaluate cognitive outcomes after ETV-CPC versus ventriculoperitoneal shunting in Ugandan infants with postinfectious hydrocephalus. The primary outcome was the Bayley Scales of Infant Development, Third Edition (BSID-3), cognitive scaled score 12 months after surgery (scores range from 1 to 19, with higher scores indicating better performance). The secondary outcomes were BSID-3 motor and language scores, treatment failure (defined as treatment-related death or the need for repeat surgery), and brain volume measured on computed tomography.
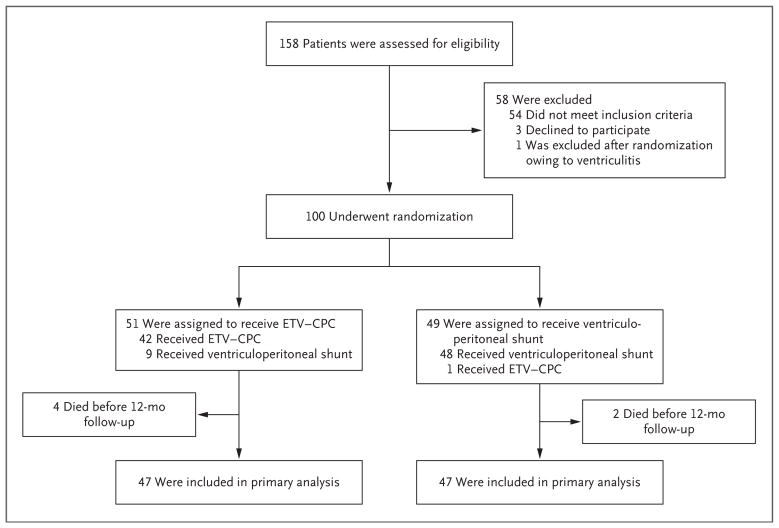
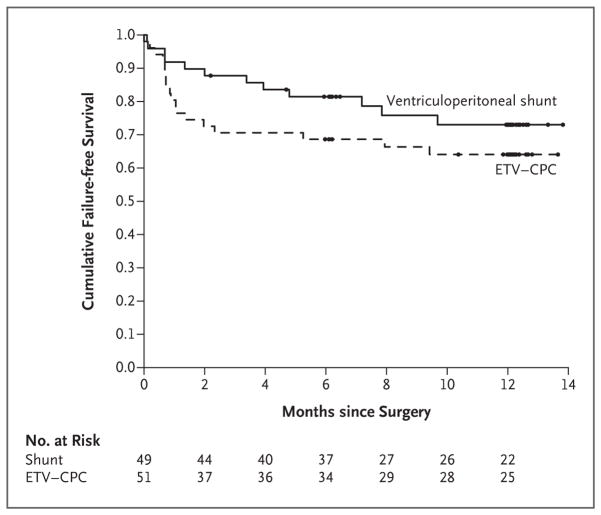
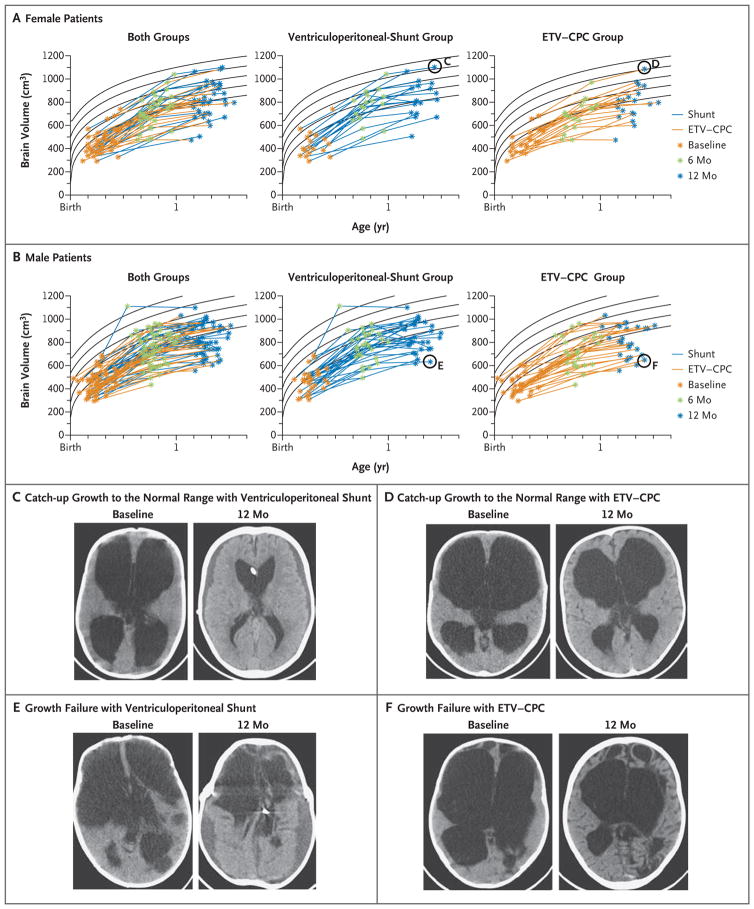
Results: A total of 100 infants were enrolled; 51 were randomly assigned to undergo ETV-CPC, and 49 were assigned to undergo ventriculoperitoneal shunting. The median BSID-3 cognitive scores at 12 months did not differ significantly between the treatment groups (a score of 4 for ETV-CPC and 2 for ventriculoperitoneal shunting; Hodges-Lehmann estimated difference, 0; 95% confidence interval [CI], -2 to 0; P=0.35). There was no significant difference between the ETV-CPC group and the ventriculoperitoneal-shunt group in BSID-3 motor or language scores, rates of treatment failure (35% and 24%, respectively; hazard ratio, 0.7; 95% CI, 0.3 to 1.5; P=0.24), or brain volume (z score, -2.4 and -2.1, respectively; estimated difference, 0.3; 95% CI, -0.3 to 1.0; P=0.12).
Conclusions: This single-center study involving Ugandan infants with postinfectious hydrocephalus showed no significant difference between endoscopic ETV-CPC and ventriculoperitoneal shunting with regard to cognitive outcomes at 12 months. (Funded by the National Institutes of Health; ClinicalTrials.gov number, NCT01936272 .).
Figures
References
-
- Warf BC. Educate one to save a few, educate a few to save many. World Neurosurg. 2013;79(2 Suppl):S15.e15–S15.e18. - PubMed
-
- Warf BC. Hydrocephalus in Uganda: the predominance of infectious origin and primary management with endoscopic third ventriculostomy. J Neurosurg. 2005;102:1–15. - PubMed
-
- Warf BC, Alkire BC, Bhai S, et al. Costs and benefits of neurosurgical intervention for infant hydrocephalus in sub-Saharan Africa. J Neurosurg Pediatr. 2011;8:509–21. - PubMed
-
- Warf BC. Comparison of 1-year outcomes for the Chhabra and Codman-Hakim Micro Precision shunt systems in Uganda: a prospective study in 195 children. J Neurosurg. 2005;102:358–62. - PubMed
-
- Lane JD, Mugamba J, Ssenyonga P, Warf BC. Effectiveness of the Bactiseal Universal Shunt for reducing shunt infection in a sub-Saharan African context: a retrospective cohort study in 160 Ugandan children. J Neurosurg Pediatr. 2014;13:140–4. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical